

Chronic spine pain treatments often fail to deliver the relief patients expect. The 2025 BMJ guidelines strongly recommend against many common interventional procedures, such as spinal injections and radiofrequency ablation, for managing chronic non-cancer spine pain. These treatments, widely used for axial (localized) and radicular (radiating) pain, show little to no benefit compared to placebo in rigorous studies.
Key Takeaways:
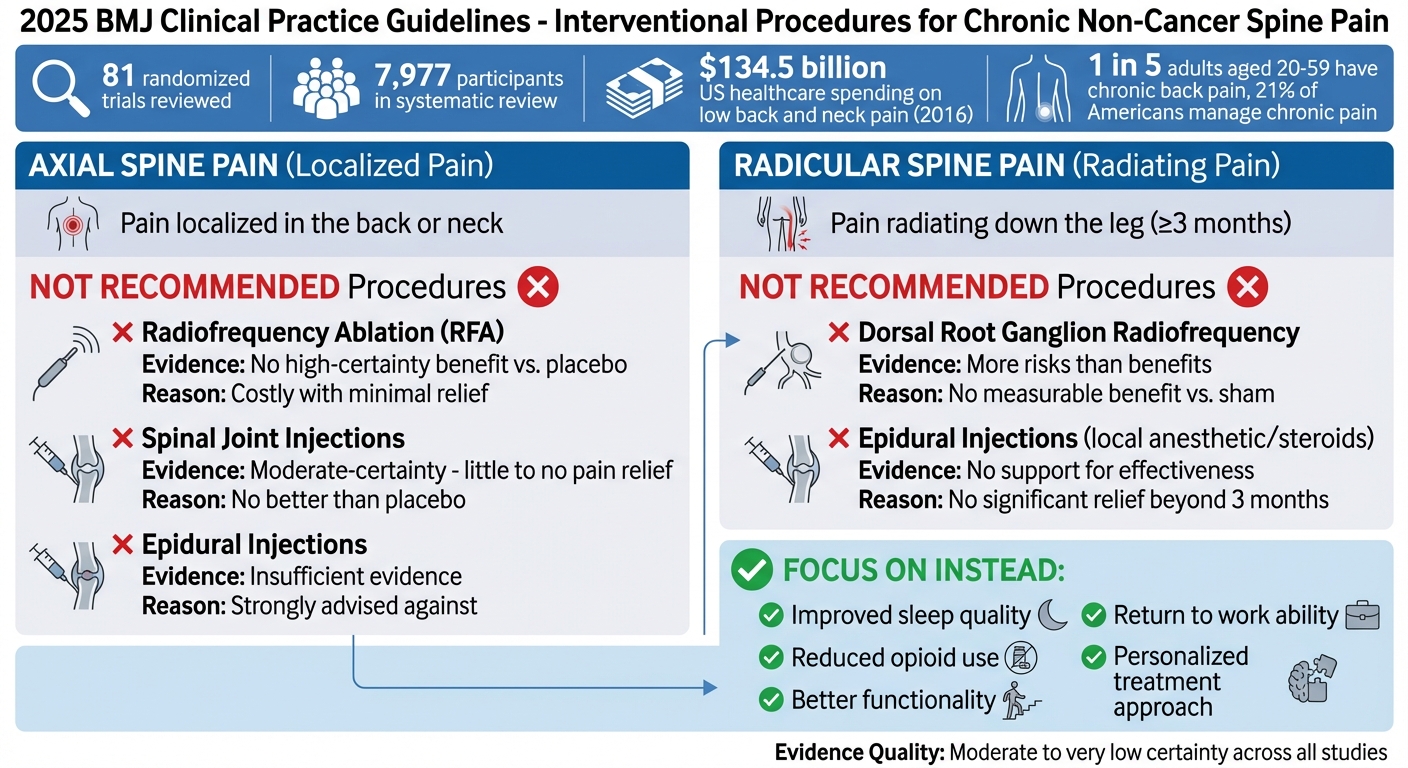
- Axial Spine Pain: Procedures like radiofrequency ablation, spinal joint injections, and epidural injections are not recommended due to minimal effectiveness.
- Radicular Spine Pain: Dorsal root ganglion radiofrequency and epidural injections also fail to show meaningful results.
- Evidence: Based on 81 trials, experts found no high-certainty benefits for these interventions.
- Focus Areas: Patients and providers should prioritize outcomes like improved sleep, reduced opioid use, and better functionality over costly, ineffective procedures.
The guidelines emphasize a personalized approach and call for better research to address gaps in treatment effectiveness.
2025 BMJ Guidelines: Interventional Procedures Not Recommended for Chronic Spine Pain
Interventional Procedures for Chronic Axial Spine Pain
Axial spine pain, as defined earlier, refers to pain localized in the back or neck. The 2025 international clinical practice guidelines recommend against the routine use of interventional procedures for this condition. Why? Because systematic reviews of randomized trials show these interventions provide little to no benefit compared to sham injections [2].
In the United States alone, healthcare spending on low back and neck pain reached a staggering $134.5 billion in 2016 [4]. A systematic review of 132 randomized trials involving 7,977 participants reinforced the conclusion: these procedures offer minimal benefit [5].
"Spine injections should not be given to adults with chronic back pain because they provide little or no pain relief compared with sham injections…" – BMJ Group [4]
Below is a closer look at the evidence behind these findings for specific procedures.
Radiofrequency Ablation for Axial Spine Pain
Radiofrequency ablation (RFA) uses radio waves to interrupt pain signals. However, systematic reviews show no high-certainty evidence that RFA provides meaningful relief compared to placebo treatments. Considering its cost and the small but present risk of harm, the guidelines strongly discourage its use – whether performed alone or alongside joint-targeted injections – for chronic axial spine pain [2][4][5].
Spinal Joint Injections for Axial Pain
Spinal joint injections involve injecting local anesthetics, steroids, or both into specific joints like the cervical or lumbar facet joints or the sacroiliac joints. The goal is to reduce inflammation and block pain signals. Yet, moderate-certainty evidence suggests these injections provide little to no actual pain relief for axial spine pain [2]. They are costly, carry minor risks (e.g., bleeding, especially in patients taking blood thinners), and perform no better than placebo treatments [4][6].
Epidural Injections for Axial Pain
Epidural injections aim to reduce inflammation and pain by delivering steroids and/or local anesthetics directly into the epidural space. However, there is insufficient evidence to support their effectiveness for chronic axial spine pain. As a result, the guidelines strongly advise against their use for this condition [2].
"…chronic pain management needs a major rethink that is perhaps best achieved by a better balance of reimbursements between procedural and non-procedural chronic pain treatments" – Jane Ballantyne, University of Washington [4]
For the estimated 1 in 5 adults aged 20 to 59 who deal with chronic back pain [4], these interventional procedures have simply not delivered the results patients and providers might hope for.
sbb-itb-ed556b0
Interventional Procedures for Chronic Radicular Spine Pain
Building on the discussion of axial interventions, current evidence suggests that interventional procedures for radicular pain often fail to deliver meaningful relief. Radicular spine pain refers to pain radiating down the leg, typically caused by nerve root compression from herniated discs or lumbar spinal stenosis. According to the 2025 BMJ Clinical Practice Guideline, commonly used interventional methods are strongly discouraged for cases of chronic radicular pain lasting three months or more.
A panel of experts analyzed data from randomized trials and found no measurable benefit when compared to placebo or sham procedures [2][10]. These recommendations specifically address non-cancer-related chronic radicular pain and mark a significant departure from earlier guidance.
"For people living with chronic radicular spine pain (≥3 months), the guideline panel issued strong recommendations against: dorsal root ganglion radiofrequency with or without epidural injection of local anesthetic or local anesthetic plus steroids; and epidural injection of local anesthetic, steroids, or their combination." – BMJ Clinical Practice Guideline [2]
Below, we explore two commonly used methods and the evidence that led to these updated recommendations.
Dorsal Root Ganglion Radiofrequency
Dorsal root ganglion (DRG) radiofrequency involves applying radiofrequency energy to the dorsal root ganglion to disrupt pain signals before they reach the brain [8]. While this approach may sound promising in theory, the 2025 guideline strongly advises against its use for chronic radicular spine pain. The data shows that DRG radiofrequency, whether performed alone or alongside epidural injections, poses more risks than benefits [10][2].
Epidural Injections for Radicular Pain
Epidural injections, often involving local anesthetics, steroids, or their combination, are another widely used intervention. However, the evidence does not support their effectiveness for chronic radicular pain lasting three months or longer [2][9]. Systematic reviews and network meta-analyses underpin the 2025 guideline’s strong recommendation against these injections. This shift underscores the urgent need for better, evidence-supported treatments for the 21% of Americans managing chronic pain [8].
What the Research Shows
The 2025 BMJ guideline recommendations are based on an in-depth analysis of 81 randomized trials, assessed through systematic reviews and network meta-analyses [1]. An international team comprising 4 patients, 10 clinicians, and 8 methodologists reviewed these trials, which spanned 13 procedures. Their conclusion? None of the procedures showed high-certainty benefits for chronic non-cancer spine pain [2][4]. Below, we break down the findings for axial and radicular procedures and discuss the limitations in existing research.
Results for Axial Spine Pain Procedures
When it comes to chronic axial spine pain, the evidence is clear: these procedures aren’t effective. Moderate-certainty evidence shows that treatments like epidural and joint-targeted injections, along with radiofrequency ablation, offer no real advantage over placebo [11][2]. Even joint radiofrequency ablation, whether performed alone or alongside joint-targeted injections, fails to provide meaningful relief [2]. Jane C. Ballantyne, a professor at the University of Washington School of Medicine, highlighted the gap between clinical practice and research findings:
"Despite the common use of spine injections in pain clinics around the world, it has been hard to come up with evidence that strongly supports this practice when applied to chronic back pain" [11].
Results for Radicular Spine Pain Procedures
The results for radicular interventions mirror those for axial pain – disappointing. Procedures like dorsal root ganglion radiofrequency and epidural injections combining local anesthetics with steroids show little to no benefit compared to sham treatments [4]. Reviews comparing these interventions to placebo found no significant relief for patients dealing with chronic radicular pain beyond three months [4].
Evidence Quality and Study Limitations
Overall, the quality of evidence supporting these procedures is limited. The certainty of findings across studies ranges from moderate to very low, making it difficult to justify their routine clinical use [2]. Even moderate-certainty evidence fails to demonstrate meaningful benefits [4]. Additionally, many studies overlook critical patient outcomes such as sleep quality, ability to return to work, and opioid usage [4]. As Ballantyne pointed out:
"The more the evidence fails to support the widespread use of these injections, the less inclined healthcare systems will be to fund them" [4].
Guideline Limitations and Research Needs
What These Guidelines Cover
These guidelines focus on managing chronic non-cancer spine pain lasting three months or longer. They specifically exclude acute pain and pain caused by conditions like inflammatory arthropathy, infections, or cancer [2]. This narrower scope means they aren’t intended for treating acute injuries or other types of pain. Keeping this in mind is essential when applying the recommendations to patient care, as the guidelines are tailored for a specific category of chronic pain.
Where More Research Is Needed
The limitations of these guidelines highlight the need for more focused research to improve treatment outcomes. The panel behind the guidelines identified several key areas that require further investigation.
One major priority is understanding whether subtypes of chronic spine pain respond differently to interventional procedures [2]. The current one-size-fits-all approach might overlook the unique needs of certain patient groups who could benefit from more customized treatments. Additionally, many procedures currently rely on evidence of low or very low certainty, making it critical to conduct stronger clinical trials to determine their actual effectiveness [2][4].
Another gap lies in the lack of attention to outcomes that directly impact patients, such as reduced opioid use, improved ability to return to work, and better sleep quality [2][4]. As noted in the BMJ publication:
"Further research is warranted and may alter recommendations in the future: in particular, whether there are differences in treatment effects based on subtypes of chronic spine pain… and effects on poorly reported patient-important outcomes (such as opioid use, return to work, and sleep quality)" [2].
Jane Ballantyne from the University of Washington also pointed out the broader implications for chronic pain management:
"This will not be the last word on spine injections for chronic back pain, but it adds to a growing sense that chronic pain management needs a major rethink that is perhaps best achieved by a better balance of reimbursements between procedural and non-procedural chronic pain treatments" [4].
Given these gaps, experts suggest that many interventional procedures should primarily be offered within the framework of clinical trials until more conclusive evidence is available [4].
Making Informed Decisions About Chronic Spine Pain
Managing chronic spine pain isn’t about following a one-size-fits-all approach. Instead, it requires collaboration between patients and healthcare providers. As Mark V. Boswell, MD, PhD, pointed out in the Pain Physician Journal:
"These guidelines do not constitute inflexible treatment recommendations. These guidelines also do not represent a ‘standard of care’" [3].
This highlights the need for a personalized approach, as every patient’s condition is unique.
The 2025 BMJ guidelines reflect this shift in thinking, strongly advising against procedures like epidural injections and joint radiofrequency ablation. Why? Evidence suggests these interventions provide minimal relief – often less than a single point on a 10-point pain scale for treatments like vertebroplasty [2][7].
When discussing treatment options with your provider, focus on outcomes that directly impact your quality of life, such as better sleep, improved work function, and reduced reliance on opioids [2]. It’s also essential to understand whether your pain is axial (confined to the spine) or radicular (spreading down your limbs), as the recommendations differ significantly between these types [2]. The BMJ panel stressed the importance of tailoring treatments to the individual, weighing the limited benefits of certain procedures against their potential risks in your specific situation [2].
This approach underscores the need for flexibility as science evolves. Some treatments might be more appropriate for clinical trials until stronger evidence is available [2]. Staying informed about new research and regularly discussing your progress with your provider will help ensure your care plan evolves alongside both medical advancements and your personal needs.
FAQs
If injections and RFA aren’t recommended, what should I try instead?
If injections and radiofrequency ablation (RFA) aren’t suitable options, there are non-invasive treatments backed by research that you can explore. These include physical therapy, consistent exercise routines, and pain management techniques. Clinical guidelines often prioritize these methods over more invasive procedures when it comes to managing chronic spine pain.
Do these guidelines apply to my sciatica or only back pain?
These guidelines address both axial spine pain and radicular spine pain, which includes conditions such as sciatica. They also discourage the use of certain interventional procedures for managing chronic pain that persists for 3 months or more. For detailed recommendations, it’s best to refer directly to the guidelines.
When might an injection still make sense for chronic spine pain?
Injections can sometimes be a useful option for managing chronic spine pain, particularly when they serve a diagnostic purpose or offer temporary relief after other treatments have not worked. That said, clinical guidelines caution strongly against using specific types of injections for chronic axial or radicular pain that has persisted for three months or more.
Related Blog Posts
- Dry cupping therapy combined with conventional therapy does not provide additional benefits over conventional therapy alone in patients with non-specific chronic low back pain: a randomized trial
- Effectiveness of Articular and Neural Mobilization for Managing Cervical Radicular Pain: A Systematic Review With Network Meta-Analysis
- Cost-effectiveness of spinal manipulation, exercise, and self-management for spinal pain
- Lumbar disc herniation: Epidemiology, clinical and radiologic diagnosis WFNS spine committee recommendations

Comments are closed