

Dealing with shoulder pain? Two popular treatments – corticosteroid injections and exercise therapy – offer different paths to relief. The SIX-Shoulder Study compared these approaches in 213 patients over 12 months. Here’s what you need to know:
- Corticosteroid injections: Provide quick pain relief (effective within 1–7 weeks) but benefits often fade after 3–6 months. Risks include mild side effects like post-injection pain and, in some cases, systemic reactions like facial flushing or menstrual irregularities. Costs are lower upfront but may require repeat treatments.
- Exercise therapy: Slower to relieve pain but matches injections in long-term results (6–12 months). It involves more time commitment (12 sessions over 12–14 weeks) but has fewer risks and supports functional recovery. Costs are slightly higher upfront.
Key takeaway: Injections are ideal for fast relief, while exercise therapy offers safer, long-term results. A combined approach – starting with injections to reduce pain and transitioning to therapy – can balance immediate relief with sustained recovery.
| Feature | Corticosteroid Injection | Exercise Therapy |
|---|---|---|
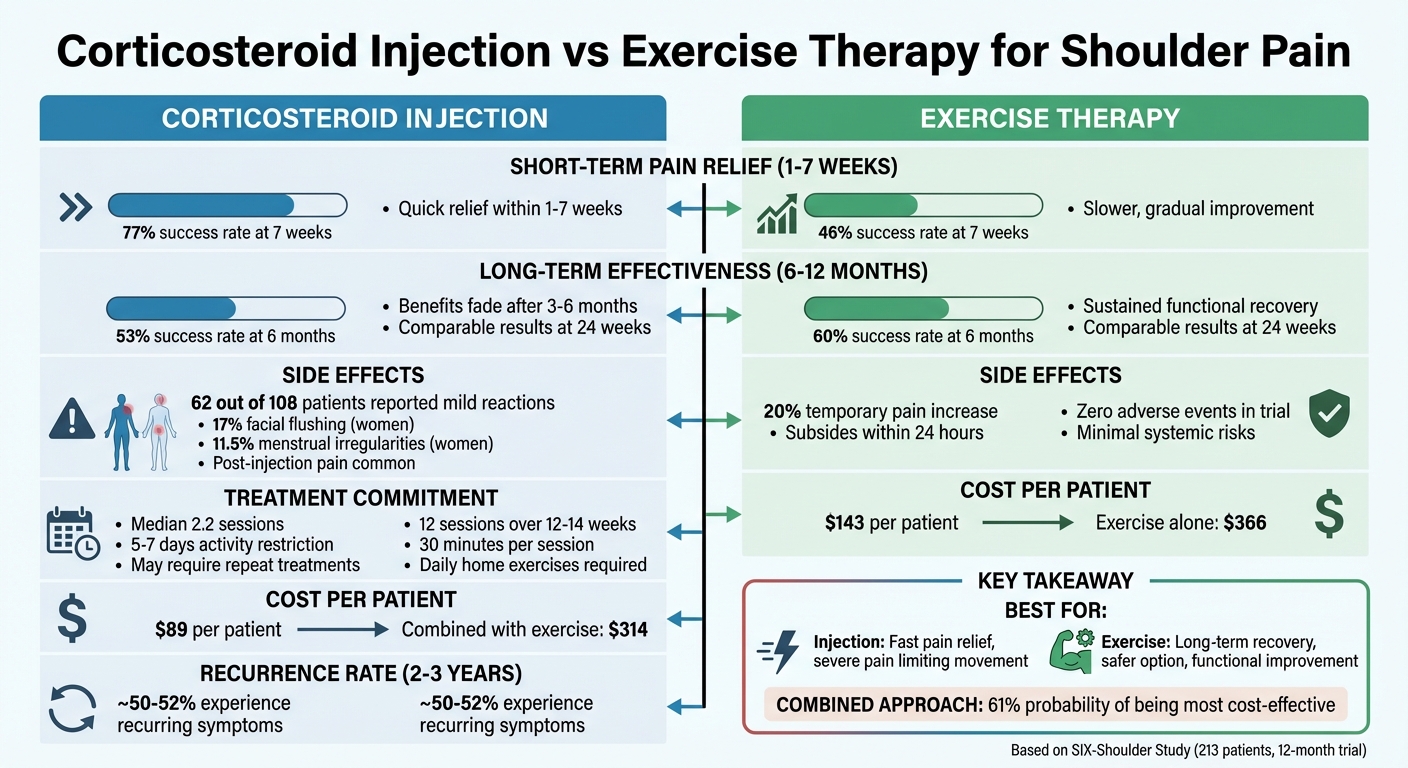
| Short-term Pain Relief | Quick (77% success at 7 weeks) | Slower (46% success at 7 weeks) |
| Long-term Effectiveness | Comparable at 6–12 months (53%) | Comparable at 6–12 months (60%) |
| Side Effects | Mild systemic risks (e.g., flushing) | Minimal (temporary pain increase) |
| Cost | ~$89 per patient | ~$143 per patient |
Choose based on your priorities: If fast pain relief is critical, injections may be the way to go. For a safer, longer-term approach, exercise therapy is a solid option.
Corticosteroid Injection vs Exercise Therapy for Shoulder Pain: Effectiveness Comparison
1. Corticosteroid Injection
Short-Term Pain Relief
Corticosteroid injections are known for providing quick relief from shoulder pain, typically within 1 to 7 weeks. A June 2010 randomized trial by Crawshaw et al., involving 232 participants with subacromial impingement syndrome, compared the combination of corticosteroid injections and exercise to exercise therapy alone. After just one week, the injection group showed a marked improvement in the Shoulder Pain and Disability Index (SPADI), with a mean difference of 6.56 (95% CI 4.30 to 8.82) [1]. By week seven, 77% of patients receiving injections were classified as treatment successes, compared to only 46% in the exercise-only group [3]. For those with synovial disorders, the outcomes were even more striking: injections led to a 75% resolution rate at five weeks, compared to 20% for physical therapy and 40% for manipulation [4].
One of the key benefits of corticosteroid injections is that they create a "window" of reduced pain, allowing patients to participate more effectively in exercise therapy [1]. This is particularly helpful for those whose moderate to severe pain hinders physical rehabilitation. Interestingly, about one-third of patients who start with exercise therapy alone may eventually require an injection, underscoring the role injections play in enabling rehabilitation during painful periods [1].
However, while the short-term results are promising, they don’t necessarily extend to long-term benefits.
Long-Term Effectiveness
The rapid relief provided by corticosteroid injections often diminishes over time. Although injections outperform exercise therapy in the short term, their benefits tend to level out by 12 to 24 weeks. In the Crawshaw trial, by week 24, there was no significant difference between the injection and exercise groups (mean difference -2.26, 95% CI -6.77 to 2.25) [1]. A systematic review further supports this, showing that while injections have a noticeable effect within six weeks, the differences often fade by the three- to six-month mark [2].
"Neither treatment is a silver bullet for functional shoulder pain and… they are likely to have some long-term problems no matter which treatment they select."
– Allen F. Shaughnessy, PharmD, MMedEd, Professor of Family Medicine [10]
Corticosteroid injections primarily address inflammation, making physical therapy more manageable, but they don’t repair tissue damage or resolve chronic conditions. Approximately 38% of patients treated with corticosteroids for shoulder impingement require additional injections within a year. Repeated use can lead to complications like cartilage degeneration, tendon weakening, and a higher risk of tendon rupture [10].
Side Effects
While effective, corticosteroid injections come with side effects. Over half of patients (62 out of 108) reported mild reactions, most commonly an increase in pain immediately after the injection [3]. Systemic reactions are more frequent in women. In a study of 53 patients, nine women reported facial flushing, and six experienced irregular menstrual bleeding, including two who were postmenopausal [3].
"Clinicians should inform female patients about the risk of irregular menstrual bleeding to prevent unnecessary anxiety or diagnostics."
– D.A.W.M. van der Windt et al. [3]
To minimize risks like tissue breakdown, it’s recommended to limit injections to three to four per year per joint, with at least three months between treatments [7][8]. Patients should avoid heavy lifting or intense activities for five to seven days post-injection [7]. Those with diabetes should monitor their blood sugar levels closely for about five days, as injections can cause temporary spikes [8][9].
Beyond the medical aspects, the financial considerations of treatment also play a role.
Cost-Effectiveness
From a cost perspective, combining injections with exercise therapy appears to be a practical choice. A UK-based trial found that the average healthcare cost per patient for an "injection plus exercise" approach was $314, compared to $366 for exercise alone [6]. With a willingness-to-pay threshold of $24,700 per quality-adjusted life year (QALY), there’s a 61% chance that the combined approach is the most cost-effective option [6].
"Injection plus exercise delivered by therapists may be a cost-effective use of resources compared with exercise alone and lead to lower health care costs and less time off work."
– Crawshaw et al., BMJ [6]
For patients seeking fast pain relief, combining a local steroid injection with physical therapy is often recommended. Clinicians should carefully monitor patients on exercise-only regimens and consider adding an injection if significant progress isn’t observed within 12 weeks [1].
sbb-itb-ed556b0
2. Exercise Therapy
Short-Term Pain Relief
Exercise therapy tends to provide slower symptom relief compared to corticosteroid injections. For example, at seven weeks, only 46% of patients who underwent physiotherapy alone were considered treatment successes, while the injection group achieved a higher success rate of 77% [3]. This highlights the delayed onset of pain relief for exercise therapy.
A trial conducted by the Leeds Musculoskeletal and Rehabilitation Service between March 2006 and August 2008 involved 232 participants aged 40 and older. Led by physiotherapist Dickon P. Crawshaw, the study revealed that 31.6% of patients (37 out of 117) in the exercise-only group eventually required additional interventions, underscoring the slower relief timeline [1].
Exercise therapy typically involves 12 sessions of 30 minutes over a 12- to 14-week period, along with home-based exercises [2]. On average, patients attended 12 sessions for physiotherapy compared to just 2.2 sessions for injections [3]. This extended time commitment, coupled with slower relief, can be particularly challenging for those experiencing moderate to severe shoulder pain.
Long-Term Effectiveness
When it comes to long-term results, exercise therapy matches or even surpasses injections. By six months, success rates (measured as a 50% reduction in disability scores) were 60% for physiotherapy and 53% for injections [5]. At the 24-week mark, there was no significant difference in the Shoulder Pain and Disability Index scores between the two treatments [1].
"Community physiotherapy and local steroid injections were of similar effectiveness for treating new episodes of unilateral shoulder pain in primary care, but those receiving physiotherapy had fewer co-interventions."
– E Hay, Staffordshire Rheumatology Centre [5]
However, long-term follow-up at two to three years shows that neither approach prevents recurrence. About 50% of patients experience recurring symptoms, emphasizing that shoulder pain often requires ongoing management rather than a one-time solution [11].
"In the long term no significant differences between the various treatment groups were found. As many as half of the patients experienced recurrent complaints."
– Jan C Winters, Department of Family Practice, University of Groningen [11]
While both treatments ultimately yield similar results, their side effect profiles set them apart.
Side Effects
Exercise therapy has minimal systemic risks, unlike corticosteroid injections. The most common issue is a temporary increase in shoulder pain following treatment. In one randomized trial, 20% of patients (11 out of 56) reported increased pain immediately after physiotherapy sessions [3]. However, this discomfort is generally mild and short-lived.
"Adverse reactions were generally mild… Few adverse reactions occurred after physiotherapy."
– D A W M van der Windt, Institute for Research in Extramural Medicine [3]
Protocols allow for some pain during or after exercises, as long as it subsides to pre-training levels within 24 hours and doesn’t disrupt sleep [2]. Unlike injections, exercise therapy avoids systemic side effects such as facial flushing or menstrual irregularities. Notably, in a trial involving 232 participants, there were zero adverse events reported in the exercise therapy group [1].
Cost-Effectiveness
Physiotherapy costs approximately $143 per patient, compared to $89 for injections – a difference of about $54 [12].
When factoring in indirect costs, the economic picture shifts. Shoulder pain generates an estimated annual cost of $4,550 per patient in primary care, with sick leave and work absences accounting for over 80% of total societal costs [2]. Additionally, only 50% of patients achieve full recovery within six months [2].
For those willing to commit to a longer treatment timeline, exercise therapy offers comparable long-term results to injections while steering clear of the risks associated with repeated steroid use. Clinicians should monitor progress closely and consider adding an injection if significant improvement isn’t achieved within 12 weeks [1]. This approach aligns with findings from the SIX-Shoulder Study, supporting exercise therapy as a solid long-term management option for shoulder pain.
Shoulder Impingement: injections vs. exercise
Advantages and Disadvantages
The table below highlights the key differences and trade-offs between corticosteroid injections and exercise therapy, based on the study’s findings.
| Feature | Corticosteroid Injection | Exercise Therapy |
|---|---|---|
| Short-term Pain Relief | Quick relief; 77% success rate at 7 weeks [3]. Most effective within the first 1–7 weeks [1][3]. | Slower improvement; 46% success rate at 7 weeks [3]. Progress builds gradually over several weeks [1]. |
| Long-term Effectiveness | Comparable to exercise at 6–12 months; 53% success rate at 6 months [5]. No notable difference in pain scores at 24–52 weeks [3][1]. | Matches injection results at 6–12 months; 60% success rate at 6 months [5]. Helps with long-term functional recovery [5][1]. |
| Side Effects | Systemic risks include 17% experiencing facial flushing and 11.5% reporting menstrual irregularities in women [3]. Local post-injection discomfort is common. | Few systemic risks. About 20% experience temporary pain increase after sessions, which usually subsides within 24 hours [3][2]. |
| Cost-Effectiveness | Lower upfront costs; typically requires a median of 2.2 sessions [3]. Combined with exercise: $255 per patient [6]. | Higher upfront costs; median of 6–12 sessions needed [1][3]. Exercise alone costs about $297 per patient [6]. 32% of patients eventually opt for injections [1]. |
| Recurrence Rate | High recurrence: about 52% of patients report symptoms returning within 2–3 years [11]. | Similar recurrence rate: about 52% of patients report symptoms returning within 2–3 years [11]. |
The findings suggest that corticosteroid injections are best for rapid pain relief, though they come with systemic side effects. On the other hand, exercise therapy provides similar long-term outcomes with fewer risks. For many patients, a combined approach – using injections for immediate relief and exercise for sustained recovery – may strike the right balance. At a willingness-to-pay threshold of $20,000 per quality-adjusted life year, there’s a 61% probability that this combined method is the most cost-effective option [6].
"If early pain relief is a priority, then adding local steroid injection to a course of physiotherapy would seem to be the best option for patients."
– Dickon P. Crawshaw, Extended Scope Practitioner Physiotherapist [1]
Despite their differences, both treatments share a similar recurrence rate, emphasizing the need for a personalized approach to shoulder pain management.
Conclusion
The SIX-Shoulder Study highlights that both corticosteroid injections and exercise therapy are effective options for managing shoulder pain, though they serve different purposes. Injections provide quick relief, making them ideal for severe pain that limits movement, while exercise therapy offers longer-term benefits and functional improvement.
Corticosteroid injections can create a "window of opportunity" by reducing pain enough to allow patients to engage in physical therapy more effectively [1]. On the other hand, for moderate pain where early function is still intact, starting with exercise therapy is often recommended. However, around one-third of patients who begin with exercise may still require an injection within three months [1]. This underscores the importance of tailoring treatment plans to each patient’s specific needs, balancing immediate pain relief with sustained recovery.
A stepped-care approach is often the best strategy. This involves starting with basic management and escalating to more intensive treatments, such as injections or structured exercise programs, as needed. Physical examinations play a crucial role in guiding treatment: for synovial disorders, injections have a treatment failure rate of about 17%, while shoulder girdle disorders often respond better to exercise and manual therapy [4].
Given that only about 50% of new shoulder pain cases fully resolve within six months [2], shared decision-making is crucial. Patients and practitioners should work together to align treatment choices with individual goals – whether that means prioritizing rapid pain relief or focusing on gradual, long-term recovery.
"Let patients know that neither treatment is a silver bullet for functional shoulder pain and that they are likely to have some long-term problems no matter which treatment they select."
– Allen F. Shaughnessy, PharmD, MMedEd [10]
FAQs
Which shoulder conditions benefit most from a steroid injection?
Corticosteroid injections are highly effective for managing shoulder conditions such as subacromial impingement syndrome and painful stiff shoulder. These injections are especially useful for alleviating pain and reducing disability in individuals experiencing moderate to severe discomfort.
When should I switch from exercises to an injection (or do both)?
Deciding how to manage shoulder pain often depends on how severe it is and how well treatments are working. If you’re dealing with moderate to severe pain that isn’t improving with exercise alone, a corticosteroid injection might offer faster relief. In some cases, combining exercise therapy with an injection can be a good option for more persistent or intense pain. It’s usually best to start with exercise therapy and, if the pain doesn’t ease up, consult your healthcare provider to figure out the most effective plan for your situation.
How many steroid shots are safe in a year for one shoulder?
It’s typically safe to get up to three or four corticosteroid injections per year in a single shoulder. Going beyond this limit could lead to potential risks like joint damage, weakened ligaments, or even osteoporosis. Be sure to consult your healthcare provider to develop a treatment plan tailored to your needs.
Related Blog Posts
- Evidence Based Kettle Bell Exercises for Shoulder Pain
- Dry needling versus cortisone injection in the treatment of greater trochanteric pain syndrome: A noninferiority randomized clinical trial
- What is the bursae denialist camp, and why is it important in relation to biomechanics and pain management?
- Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging

Comments are closed