

Did you know that nearly everyone over 40 has rotator cuff abnormalities on MRI – even without pain? Studies show that 98.7% of adults aged 41–76 have detectable changes, like tendinopathy or tears, regardless of symptoms. These findings suggest most abnormalities are part of normal aging, not necessarily the cause of shoulder pain.
Key points from the research:
- 96% of symptom-free individuals still show abnormalities on MRI.
- Full-thickness tears increase with age, affecting 28% of people by 70.
- The difference in tear rates between painful and pain-free shoulders is only 0.8% after adjusting for age.
- Many abnormalities are harmless and don’t require treatment.
This challenges the idea that every MRI finding needs fixing. Instead, treatment should focus on symptoms and improving shoulder function through conservative care like physical therapy. Imaging is best used to confirm – not drive – diagnoses, ensuring patient care is tailored to individual needs.
Demystifying the Shoulder MRI, What chatGPT Won’t Tell You | Brian Feeley, MD
Research Data on Rotator Cuff Abnormalities
Rotator Cuff Abnormalities by Age: MRI Findings in Symptomatic vs Asymptomatic Shoulders
Study Results and Prevalence Numbers
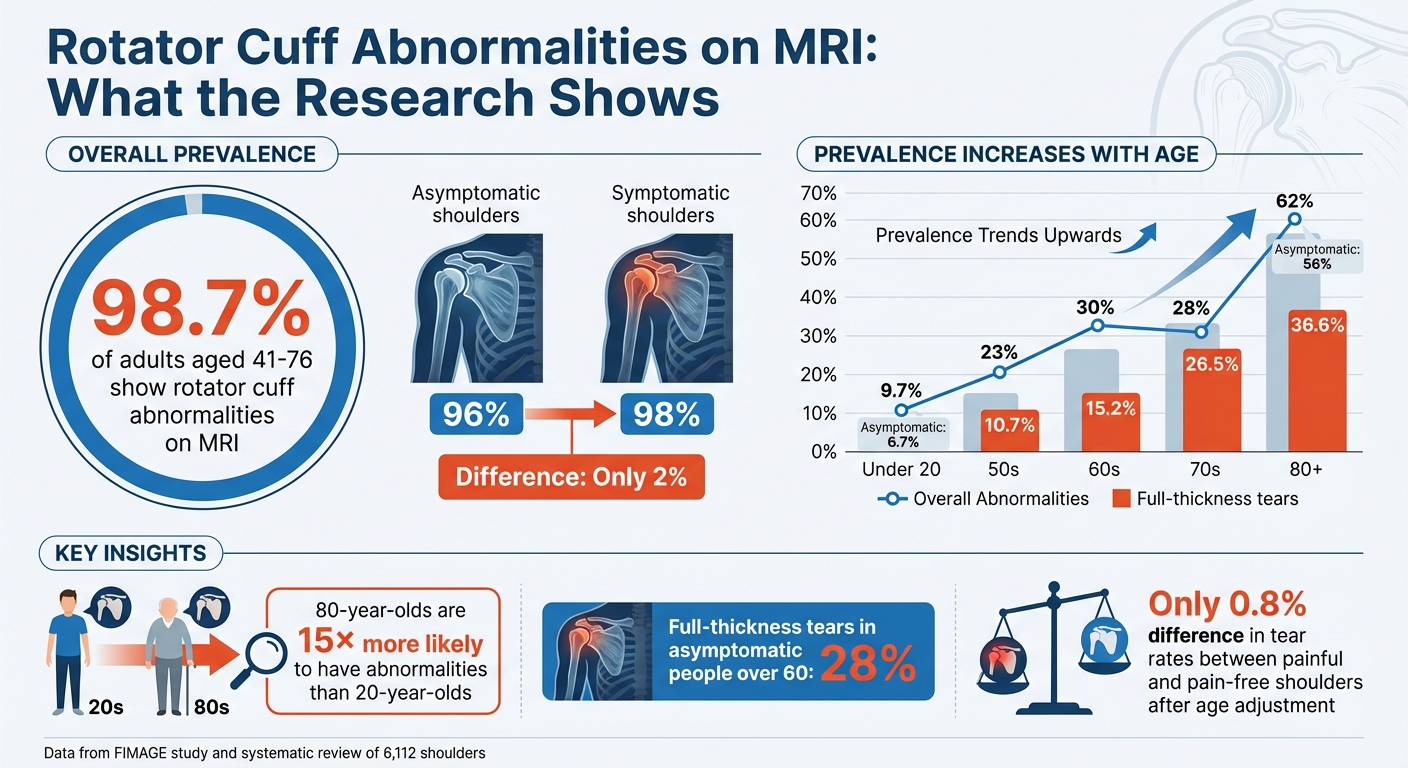
The FIMAGE study reveals that rotator cuff abnormalities are almost universal in adults over 40. Among asymptomatic shoulders, abnormalities were found in 96% of cases, compared to 98% in symptomatic shoulders – a mere 2% difference [1]. This small gap indicates that structural changes alone don’t necessarily lead to symptoms.
A larger systematic review, which analyzed 6,112 shoulders across multiple studies, showed that the prevalence of rotator cuff abnormalities rises with age. In individuals under 20, the rate is 9.7%, but it jumps to 62% in those aged 80 and above [6]. For asymptomatic individuals, the prevalence climbs from 6.7% in those over 20 to 56% in the 80-plus age group [6]. These findings highlight the importance of evaluating patients in context, as imaging alone often doesn’t tell the full story.
Age and Sex Patterns
Age plays a major role in the likelihood of detecting rotator cuff abnormalities on MRI. An 80-year-old is 15 times more likely to have these abnormalities compared to a 20-year-old [6]. Full-thickness tears, in particular, show a pronounced age-related increase. They are rare in individuals under 45 but rise to 28% in those 70 and older [3]. The progression is clear: tear rates climb from 10.7% in people in their 50s, to 15.2% in their 60s, 26.5% in their 70s, and 36.6% in their 80s [5].
As for sex differences, recent studies using advanced 3-Tesla MRI technology show that gender does not significantly impact the prevalence of these abnormalities [1]. While older research suggested men in their 50s and 60s had higher tear rates, newer data confirms that prevalence and severity are consistent between men and women across all age groups [1]. These findings emphasize the need to focus on broader factors when interpreting imaging results.
How Imaging Findings Relate to Symptoms
Research consistently shows a weak link between MRI findings and clinical symptoms. For adults over 40, tendinopathy and partial-thickness tears are just as common in asymptomatic shoulders as in symptomatic ones [3]. Full-thickness tears are slightly more prevalent in symptomatic shoulders (14.6% vs. 6.5%), but this association diminishes significantly when age and other variables are considered [1].
In individuals over 60, about 54% of asymptomatic people have rotator cuff tears, with 28% showing full-thickness tears and 26% having partial-thickness tears [8]. These findings suggest that such structural changes are a natural part of aging rather than a sign of pathology requiring intervention.
"The results of the present study emphasize the potential hazards of the use of magnetic resonance imaging scans alone as a basis for the determination of operative intervention in the absence of associated clinical findings." – Sher et al., PubMed Abstract [8]
This disconnect between imaging results and symptoms underscores the importance of a comprehensive clinical evaluation. Patient history, physical exams, and assessments of functional limitations should guide treatment decisions, rather than relying solely on MRI findings [3][4]. This evidence supports a more cautious and individualized approach to clinical care, which will be explored further in the next section.
How to Use MRI Results in Patient Care
Treat the Person, Not the Picture
Here’s a striking fact: 98.7% of adults aged 41 to 76 show at least one rotator cuff abnormality on MRI, regardless of whether they feel shoulder pain or not [3][1]. This highlights an essential truth – imaging alone doesn’t tell the whole story. To truly help patients, you need to focus on their specific symptoms, movement challenges, and personal goals, rather than getting lost in what the scan shows.
"Management decisions should be guided by history, physical examination, and functional limitation." – Edgar Garcia-Lopez, MD and Brian T. Feeley, MD, UCSF Department of Orthopedic Surgery [3]
For example, when a patient reports shoulder pain, their ability to reach overhead, sleep comfortably, or lift objects matters more than the abnormalities visible on their MRI. It’s important to remember that many people with significant imaging findings feel no pain, while others with minor changes can experience severe discomfort. Treatment should aim to reduce symptoms and improve function, not necessarily "fix" every abnormality on the scan.
Once you’ve established this patient-centered approach, you can combine your clinical insights with imaging results for more informed decisions.
Step-by-Step Clinical Decision-Making
Start by taking a detailed history and performing a focused physical exam to pinpoint movement issues and triggers for pain. For patients with atraumatic shoulder pain, experts suggest trying 6 to 8 weeks of conservative therapy – like physical therapy or injections – before considering advanced imaging [3][9]. This approach helps avoid unnecessary interventions. Interestingly, research shows that 36% of patients who had an MRI for shoulder pain had not tried any conservative treatments beforehand [9], indicating that imaging is often ordered too soon.
"MRI may be useful to confirm but not establish a diagnosis and could be used to help plan a surgical intervention rather than determine whether surgery is going to be helpful." – Edgar Garcia-Lopez, MD and Brian T. Feeley, MD [3]
Use MRI as a tool to confirm your clinical suspicions, not as the first step in diagnosis. If a patient doesn’t respond to conservative care or if trauma suggests surgery might be needed, imaging can help refine your plan. Pay close attention to specific MRI findings that are more likely linked to symptomatic tears, such as tears larger than 3 cm in the medial-lateral plane, severe muscle atrophy (positive tangent sign), or advanced fatty degeneration (Goutallier grade 2–4) in the supraspinatus or infraspinatus muscles [7].
How to Explain Findings to Patients
Once you’ve reviewed the MRI and clinical findings, clear communication with your patient becomes key. Many patients feel anxious about imaging results, so it’s crucial to frame the information in a way that reduces worry. For instance, instead of saying, “You have a tear,” you might explain, “Your MRI shows age-related changes that are found in 96% of people your age who don’t have shoulder pain” [3][1]. Comparing these findings to "wrinkles on the inside" or "gray hair" often helps patients understand that such changes are a normal part of aging and don’t always need treatment.
"Clinical correlation with history and physical examination is critical to differentiate between anatomic variants, incidental findings, and true pathology." – Jenny T. Bencardino, MD, NYU Hospital for Joint Diseases [2]
It’s also worth explaining that certain technical artifacts, like the "magic angle" effect, can mimic problems on an MRI. If the report mentions mild signal changes, reassure patients that these might not indicate real damage. Shift the focus away from the imaging report and toward their functional goals – what they want to achieve and how you’ll work together to get there. This approach helps patients stay engaged and optimistic about their recovery.
sbb-itb-ed556b0
Treatment Options for Incidental Findings
When it comes to managing incidental findings, the focus remains on preserving shoulder function and promoting long-term health through patient-centered care.
Prevention Strategies for Asymptomatic Findings
If an MRI reveals rotator cuff issues without symptoms, the goal is to maintain a healthy shoulder and prevent future problems. The key lies in maintaining mobility, improving posture, and building strength through active movement. Start with self-mobilization exercises and gentle stretches to ensure your shoulder joint stays flexible. Pay attention to scapular mechanics – correcting protraction can improve the subacromial space and reduce the risk of impingement [10][11].
Posture is often overlooked but plays a crucial role. Spending long hours hunched over a desk or staring at screens can cause your shoulders to roll forward, putting unnecessary strain on the rotator cuff. Simple postural reeducation and scapular-control exercises can help your shoulder blade move properly during arm movements, reducing stress on the rotator cuff [10].
Conservative Care for Mild Symptoms
For mild shoulder discomfort, a structured rehabilitation program is usually the first step. Conservative treatments are effective for most cases, boasting success rates of 73% to 80% for full-thickness rotator cuff tears [11]. These programs typically progress based on symptom improvement [10].
Rehabilitation unfolds in phases. Initially, the focus is on managing pain and inflammation with gentle mobility exercises, posture correction, and possibly a short course of anti-inflammatory medication. As symptoms improve, isometric exercises and low-load strengthening are introduced, with care taken to avoid flare-ups. The final stages involve progressive loading, including eccentric exercises, isokinetic training, Blood Flow Restriction (BFR) training, and kinetic-chain movements that engage the entire body [10]. This phased approach works particularly well for conditions like tendinopathy or small tears affecting less than 50% of the tendon thickness [10].
When to Refer for Further Evaluation
While most shoulder conditions respond well to conservative care, some cases require specialist attention. If symptoms persist beyond 12 weeks of targeted strengthening, a referral is advisable [10]. Other red flags include acute traumatic tears involving more than 50% of the tendon, retracted tears where the tendon pulls away from the bone, or significant muscle atrophy – especially in younger or very active individuals [10].
Surgery is typically delayed in conditions like adhesive capsulitis (frozen shoulder) until range of motion improves or when cervical radiculopathy (nerve-related pain originating from the neck) is the root cause of discomfort [10]. During rehabilitation, follow-up ultrasounds every 3 to 6 weeks may be used to monitor tendon remodeling and ensure the tear isn’t worsening [10]. It’s worth noting that 51% of asymptomatic tears become symptomatic within an average of 2.8 years, with symptoms often linked to an increase in tear size [11]. These strategies pave the way for tailored care, which will be discussed further in the next section on how Portland Chiropractic Group can assist.
How Portland Chiropractic Group Can Help

Using Research to Guide Treatment
At Portland Chiropractic Group in Oklahoma City, treatment is grounded in research-backed insights. For example, studies reveal that 96% of asymptomatic shoulders show at least one rotator cuff abnormality [3]. As Thomas Ibounig, MD, from the Finnish Centre for Evidence-Based Orthopaedics, explains:
"MRI examination of the shoulder found that [rotator cuff] abnormalities are present in nearly all individuals over 40 years of age, irrespective of symptoms." [3]
This highlights the importance of focusing on the patient as a whole rather than relying solely on imaging results. A thorough physical exam evaluates how your shoulder moves, pinpoints areas of weakness, and identifies whether other regions, such as the upper back or ribs, might be contributing to the problem. This approach helps reduce unnecessary worry over findings that may simply reflect natural aging. These insights directly shape personalized, hands-on treatment plans.
Available Treatment Options
The clinic follows evidence-based guidelines for conservative care, aiming to restore function and ease discomfort. Treatment options include chiropractic adjustments, the Graston technique, dry needling, shockwave therapy, and functional training. Here’s how some of these methods work:
- Graston technique: This method helps break down scar tissue and improve soft tissue mobility.
- Dry needling: Targets trigger points and tight muscles, improving flexibility and reducing pain.
- Shockwave therapy: Uses acoustic waves to promote healing in damaged tendons.
Functional training plays a key role in correcting movement patterns that contribute to shoulder strain. These exercises focus on improving scapular control, strengthening rotator cuff muscles, and restoring smooth coordination between the shoulder blade and arm. The clinic’s open floor plan fosters transparency in care, while private consultations provide a comfortable space for more personal discussions.
Building Long-Term Shoulder Health
Portland Chiropractic Group doesn’t just focus on immediate relief – it also prioritizes long-term shoulder wellness. Preventing future issues means addressing the entire system, not just the rotator cuff. As Portland Chiropractic Neurology puts it:
"Addressing all structures involved in pain is essential for… healthy function." [13]
Wellness programs are designed to maintain mobility and strength over time. These include postural education, movement assessments to catch potential problems early, and ongoing maintenance care to prevent minor issues from escalating. With nearly 70% of people experiencing shoulder problems at some point [12], taking proactive steps now can help keep your shoulders healthy and functional for years to come.
Conclusion: Main Points for Managing Rotator Cuff Abnormalities
Here’s the bottom line: MRI findings alone shouldn’t dictate treatment decisions. Studies reveal that 98.7% of adults aged 41 to 76 show at least one rotator cuff abnormality on MRI, whether they have shoulder pain or not [3][1]. These changes often reflect normal aging, not a condition that requires medical intervention.
The focus should always be on the patient’s symptoms, functional challenges, and physical exam results. After accounting for demographic factors, the difference in full-thickness tears between symptomatic and asymptomatic shoulders is just 0.8% [3][1]. This highlights how imaging results, on their own, have limited value in guiding care.
For non-traumatic shoulder pain, starting with 6 to 8 weeks of conservative care – like strengthening, mobility exercises, and scapular control – can help avoid overdiagnosis and unneeded treatments [3]. This approach prioritizes improving shoulder function without jumping straight to advanced imaging or invasive procedures.
Understanding that many rotator cuff changes are part of normal aging can ease patient concerns and shift the focus to what really matters: how the shoulder feels and works. Treating the person, not just the scan, leads to better outcomes and fewer unnecessary interventions [3][1].
FAQs
If MRI findings are common, what actually causes shoulder pain?
Shoulder pain is frequently associated with structural issues such as rotator cuff tears larger than 3 cm, a positive tangent sign, and fatty degeneration of the rotator cuff muscles. These factors tend to play a bigger role in causing symptoms compared to incidental findings on an MRI.
When should I get an MRI for shoulder pain?
If shoulder pain lingers despite treatment or initial tests like X-rays fail to pinpoint the problem, an MRI might be worth considering. MRIs are particularly useful for spotting soft tissue problems, such as rotator cuff tears or tendon injuries, which are common in chronic shoulder issues. However, keep in mind that MRIs can sometimes uncover unrelated findings, so the results should always be evaluated alongside your symptoms. Talk to your healthcare provider to determine if an MRI makes sense for your situation.
What symptoms mean a rotator cuff tear needs surgery?
If you’re dealing with ongoing shoulder pain, weakness, or a restricted range of motion that isn’t getting better with non-surgical treatments, surgery for a rotator cuff tear might be necessary. Surgery becomes even more critical if the tear worsens over time or starts to seriously affect your ability to perform everyday tasks.
Related Blog Posts
- Why Is Fatty Infiltration in the Multifidi Muscle Important for a Chronic Low Back Pain Prognosis?
- Association between cervical MRI findings and patient-reported severity of headache in patients with persistent neck pain: a cross-sectional study
- Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain
- Lumbar disc herniation: Epidemiology, clinical and radiologic diagnosis WFNS spine committee recommendations

Comments are closed