

When someone tears their ACL and opts out of surgery, the surrounding thigh muscles – especially the hamstrings – gradually weaken over time, impacting knee stability and increasing the risk of early osteoarthritis. A recent 4-year study of 1,207 patients, led by Johns Hopkins researchers, revealed key insights:
- Hamstrings shrink by –28.18 mm² and lose –3.49 N of strength annually in ACL-deficient knees.
- Quadriceps remain stable after the initial injury phase, while posterior thigh muscles deteriorate.
- Early rehab should focus on quadriceps recovery, but long-term care must prioritize hamstring preservation.
These findings emphasize the importance of tailored rehabilitation strategies, especially for patients managing ACL injuries without reconstruction. Strengthening the hamstrings and monitoring muscle health can help maintain knee stability and delay joint degeneration.
Study Design and Methods
Patient Selection and Demographics
Participants for this study were drawn from the Osteoarthritis Initiative (OAI) and had ACL tears confirmed through MRI scans. Importantly, none of the participants had undergone ACL reconstruction, allowing researchers to observe the natural progression of an ACL tear over time [4].
To ensure balanced comparisons, researchers used propensity score matching in ratios of 1:2 to 1:3. This approach paired each ACL-deficient thigh with ACL-intact control thighs that matched in terms of age, weight, and activity level. The final dataset included 92 ACL-deficient thighs and 1,115 ACL-intact control thighs, for a total of 1,207 thighs. The average age of participants was 61 ± 9 years, and all were monitored over a 4-year period [4]. This careful selection process provided a strong foundation for the MRI and strength assessments that followed.
MRI Measurements of Muscle Tissue
The study utilized advanced 3T MRI scanners to capture detailed images of muscle tissue and fat distribution. T1-weighted spin-echo sequences were used to measure muscle cross-sectional area and volume at 33% of the femoral length from the knee [5][2]. A validated deep-learning model automatically segmented muscle groups and calculated two key metrics: intra-muscular adipose tissue (IMAT) and the percentage of contractile tissue. Fat infiltration within the muscles was assessed using the Goutallier Classification, a five-point scale ranging from Grade 0 (normal) to Grade 4 (more than 50% fat) [7][2][4].
Following the imaging analysis, researchers also evaluated muscle strength using standardized testing protocols.
Strength Testing Protocols and Data Analysis
Muscle strength was assessed using specialized equipment, including the Good Strength Chair (Metitur Oy) and the Biodex System 3. Participants performed three 3-second maximal voluntary isometric contractions (MVICs) at knee flexion angles of 60° and 90°. The highest value recorded during these tests was used as the official measurement [6].
To analyze the data, researchers applied linear mixed-effects models, which allowed them to track changes over time while accounting for individual variability. Specific strength was calculated by dividing absolute force (measured in Newtons) by the MRI-measured muscle cross-sectional area [5][4].
This comprehensive methodology provided a clear view of how thigh muscles evolve over time in ACL-deficient knees.
Main Findings from the Study
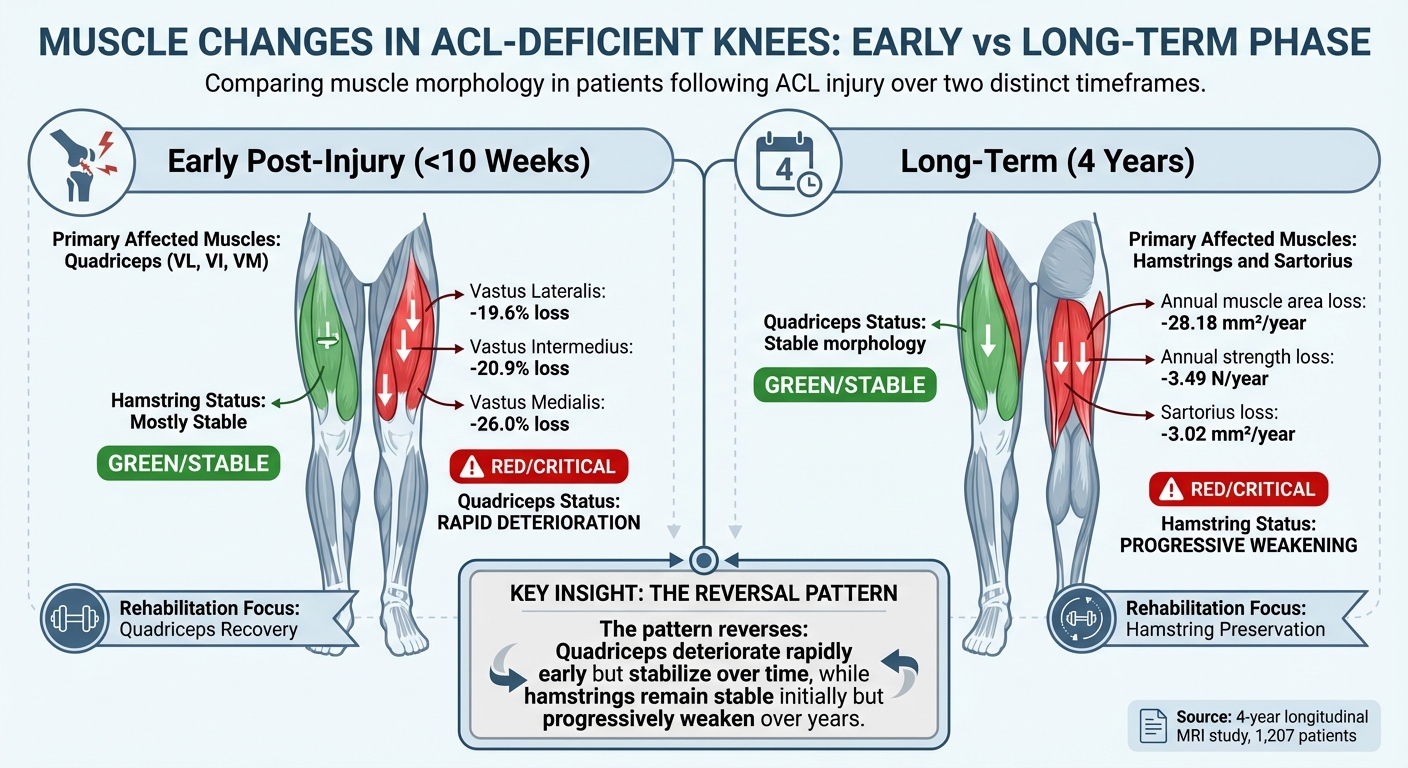
ACL Injury Muscle Changes: Early vs Long-Term Phase Comparison
Changes in Muscle Composition Over 4 Years
Over a four-year period, ACL-deficient knees showed a specific pattern of muscle deterioration, primarily affecting the posterior thigh muscles. The hamstrings experienced an annual atrophy of –28.18 mm², while the sartorius declined by –3.02 mm² per year [4]. In contrast, the quadriceps and adductor muscles showed no significant changes in cross-sectional area when compared to healthy knees. Interestingly, fat infiltration levels remained consistent between ACL-deficient and healthy knees, suggesting that the issue lies in the gradual loss of muscle tissue in targeted areas, not in the overall quality of the muscle [4].
"The present findings highlight selective muscle deterioration in the posterior thigh muscles following ACL injury, with minimal changes in quadriceps morphology, over time." – Osama Alzobi, MD, Department of Orthopaedic Surgery, Hamad Medical Corporation [4]
Progressive Hamstring Strength Loss
Beyond muscle size reduction, the hamstrings also showed a measurable decline in strength, losing –3.49 N per year [4]. This weakening further compromises knee stability, especially in an ACL-deficient knee. The combined effect of reduced muscle size and strength exacerbates the challenge, particularly during activities requiring sudden stops or rapid directional changes.
Long-Term Changes vs. Early Post-Injury Patterns
The four-year trends in muscle changes differ significantly from what happens shortly after an ACL injury. In the first 10 weeks post-injury, the quadriceps experience the most severe impact, with the vastus lateralis shrinking by 19.6%, the vastus intermedius by 20.9%, and the vastus medialis by 26.0% [1]. During this early phase, the hamstrings remain relatively unaffected. However, over the years, this pattern shifts. Quadriceps losses stabilize, while the hamstrings progressively weaken, both in size and strength [4]. These evolving dynamics underscore the need to adjust rehabilitation strategies to address long-term changes effectively.
| Phase | Primary Affected Muscles | Quadriceps Status | Hamstring Status |
|---|---|---|---|
| Early Post-Injury (<10 Weeks) | Quadriceps (VL, VI, VM) [1] | Significant size and quality loss [1] | Mostly stable [1] |
| Long-Term (4 Years) | Hamstrings and Sartorius [4] | Stable morphology [4] | Progressive atrophy and strength loss [4] |
Recognizing these distinct phases is essential for designing rehabilitation programs that prioritize preserving knee stability and addressing the specific needs of each stage.
How These Findings Apply to Patient Care
The detailed MRI findings provide a strong foundation for improving patient care, particularly for those with ACL injuries. Here’s how this evidence translates into actionable strategies.
Effects on Knee Function and Joint Health
ACL-deficient knees experience significant hamstring atrophy, with a loss of –28.18 mm² in muscle area and –3.49 N of force annually, which compromises dynamic knee stability[4]. The hamstrings play a key role in limiting anterior tibial translation, compensating for the torn ACL[1]. Maintaining a larger thigh muscle cross-sectional area is critical for reducing the risk of joint degeneration and delaying osteoarthritis onset[2]. Additionally, the sartorius muscle, which atrophies by –3.02 mm² annually, provides medial knee stability, and its decline may contribute to faster joint deterioration[4].
Rehabilitation Strategies for ACL-Deficient Knees
The progression of muscle changes after ACL injuries highlights the importance of a phased rehabilitation plan. During the first 10 weeks post-injury, the focus should be on the quadriceps, which can lose 19.6% to 26.0% of their physiological cross-sectional area in this period[1]. After the acute phase, the emphasis shifts to preserving hamstring strength through eccentric exercises, deadlifts, and neuromuscular training. These practices address motor unit recruitment challenges that can persist for up to a year[8].
"Patients may benefit from exercises aimed at improving quadriceps cross-sectional area post-operatively." – Abbey C. Thomas, PhD, ATC[6]
Bilateral training is equally important. Quadriceps activation deficits are often seen in both the injured limb (13%) and the uninjured one (15%), well above the healthy threshold of 5%[6]. This makes addressing both sides essential for recovery.
Applying These Findings at Portland Chiropractic Group

At Portland Chiropractic Group, these insights are directly applied to patient care through tailored interventions. Chiropractic adjustments are used to maintain proper joint mechanics and minimize compensatory movement patterns that could worsen muscle loss. Soft-tissue techniques, such as the Graston technique and dry needling, target quadriceps fibrosis, as MRI findings frequently confirm its presence[1].
Our functional training programs prioritize progressive hamstring strengthening, acknowledging that atrophy may continue for up to four years without intervention[4]. Additional therapies include neuromuscular electrical stimulation to counter early muscle inhibition, blood flow restriction therapy to encourage muscle growth while reducing joint strain, and cross-education techniques that utilize the uninjured limb to speed up recovery[10]. This comprehensive, evidence-based approach ensures both immediate and long-term patient outcomes are addressed effectively.
sbb-itb-ed556b0
Managing Muscle Changes After ACL Injury: Practical Steps
What to Monitor in Long-Term Care
To effectively track recovery after an ACL injury, isokinetic dynamometry at 60°/second is a reliable tool for assessing knee flexor and extensor strength. Additionally, monitoring muscle cross-sectional area and activation through the Central Activation Ratio (CAR) is critical. CAR helps determine whether strength loss is due to muscle atrophy or arthrogenic muscle inhibition – a condition where the central nervous system struggles to fully activate the muscle [3][8].
For patients managing their injury without surgery, the focus of monitoring evolves after the early recovery phase. While quadriceps morphology tends to stabilize, hamstring deterioration often continues over time [4]. Testing should also include the uninjured leg, as neural activation deficits can affect both limbs [3].
"Monitoring the strength of the muscle is a useful practice when evaluating the progression of recovery. However, clinicians can also consider the deficits in muscle activation."
– University of Florida Research Team [3]
These insights help guide the exercise programs outlined in the next section.
Exercises and Training Methods That Work
Strength training with loads exceeding 80% of one-repetition maximum is crucial for addressing arthrogenic muscle inhibition by boosting neural drive [8]. This approach is especially important because motor unit recruitment remains altered for at least a year post-injury. Even after returning to sport, smaller motor units are often favored, which can hinder optimal muscle performance [8].
Incorporating ballistic and power exercises can help lower motor unit recruitment thresholds, improving overall force development [8]. To specifically target hamstring strength and counteract long-term muscle loss, the Nordic Hamstring Exercise is highly effective at enhancing eccentric knee flexor strength [9].
For patients who opt out of ACL reconstruction, these exercises become even more essential to their rehabilitation.
Care Considerations for Patients Without ACL Reconstruction
For those managing an ACL injury without surgery, rehabilitation priorities shift. Long-term care should focus more on hamstring strengthening, as opposed to the quadriceps-centered strategies often used in post-surgical recovery.
Neuromuscular training and dynamic stability exercises are key for these patients, particularly since reinjury rates can reach up to 33% within two years [8]. Additionally, rehabilitation should include testing and strengthening of the hip extensors, hip adductors, and ankle plantar flexors, as these muscle groups often weaken following an ACL injury and are essential for maintaining knee stability [11]. These targeted strategies support joint health and functional recovery in the long term.
Conclusion: What This Means for ACL-Deficient Patients
This study sheds light on the ongoing challenges and potential solutions for managing ACL-deficient knees. One key takeaway is that quadriceps muscles deteriorate rapidly within 10 weeks of injury, while hamstring muscles weaken progressively at a rate of -28.18 mm²/year in non-surgical cases [4]. These findings emphasize the importance of developing rehabilitation strategies that adapt to the different phases of recovery.
Perhaps the most crucial insight is that maintaining high thigh muscle mass can help protect against early osteoarthritis, regardless of whether surgery is part of the treatment plan [2]. Research suggests that a larger thigh muscle cross-sectional area may play a protective role against degenerative knee changes, independent of ACL status. This means your rehab approach should evolve over time – starting with quadriceps preservation immediately after the injury and transitioning to a focus on hamstring strengthening for long-term management, especially in cases where surgery is not pursued.
"High thigh muscle CSA is associated with less degenerative changes at the knee, independent of the ACL status and may potentially be advantageous in the prevention of early OA." – Jungmann PM, et al. [2]
At Portland Chiropractic Group, we integrate these findings into a personalized approach for every patient. Whether you’re preparing for surgery, recovering afterward, or managing your knee without reconstruction, targeted rehabilitation ensures the right muscles are prioritized at the right time. Early intervention is critical, as muscle quality begins to decline within weeks of injury. A well-designed plan that addresses both muscle strength and composition can improve recovery outcomes and reduce the risk of future complications. These insights bridge the gap between research and patient care, offering a roadmap for effective long-term knee health.
FAQs
Why do hamstrings weaken over time in an ACL-deficient knee?
Hamstring weakness in an ACL-deficient knee happens because the muscles adapt and shrink after the injury. As they try to compensate for the damaged ligament, their strength gradually diminishes over time. This underscores the need for focused rehabilitation to help restore muscle strength and proper function.
What hamstring exercises best improve knee stability without ACL surgery?
To help improve knee stability without ACL surgery, it’s important to strengthen your hamstrings, as they play a key role in supporting the knee joint. Some effective exercises to target this muscle group include hamstring curls, Romanian deadlifts (RDLs), bridges, and the Nordic hamstring exercise. These movements not only build strength but also boost endurance, which helps stabilize the knee and lowers the risk of further injury. Adding these exercises to a rehabilitation routine can support knee function and reduce instability over time.
How can I track thigh muscle loss after an ACL tear?
You can monitor thigh muscle loss following an ACL tear with imaging tools such as MRI or CT scans. These techniques provide detailed measurements of the muscle’s cross-sectional area and quality, making it possible to track atrophy and structural changes over time. Regular imaging is especially useful for assessing the quadriceps, which are often heavily affected by ACL injuries, and can help gauge the success of rehabilitation efforts.
Related Blog Posts
- Why Is Fatty Infiltration in the Multifidi Muscle Important for a Chronic Low Back Pain Prognosis?
- Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain
- Effectiveness of fascial manipulation® versus eccentric training with static stretching on patellar tendinopathy – A randomized clinical trial
- Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging

Comments are closed