

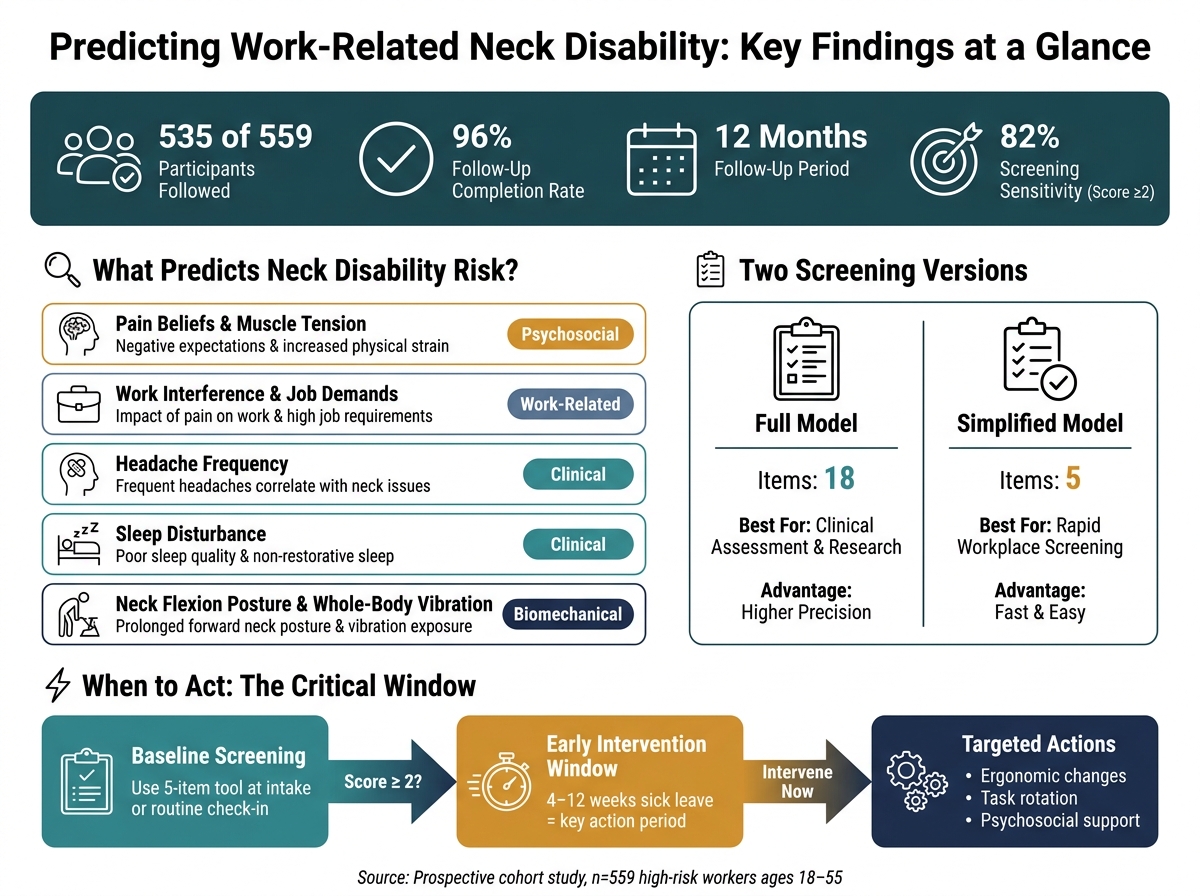
I found the main takeaway simple: workers in high-risk jobs can be screened early for 12-month neck disability using a short set of baseline factors. In this study, 535 of 559 workers finished follow-up (96%), and the short screening version flagged most at-risk workers with 82% sensitivity when the score was 2 or higher.
Here’s what matters most if you want the short version:
- The goal: estimate who may develop work-related neck disability within 12 months
- Who was studied: full-time workers ages 18–55 in jobs with high neck strain
- How disability was defined: neck pain lasting more than 24 hours, pain over 30/100, NDI 5 or higher, and no neurologic symptoms
- What predicted risk: pain beliefs, work interference, headaches, sleep problems, baseline pain, neck-flexed work posture, and whole-body vibration
- Why it matters: early screening can guide job changes, workstation fixes, support, and care planning
What stood out to me is this: risk was not just about posture. The model points to a mix of symptoms, sleep, work strain, and beliefs about pain. That gives clinicians and employers a more useful starting point than looking at body position alone.
If I were explaining the study in one line, I’d say this: a short screening tool may help catch workers headed toward chronic neck-related work limits before the problem gets worse.
Neck Disability Risk Screening: Key Stats & Predictors at a Glance
Neck Disability Index (NDI) explained | Step-by-Step Scoring & Clinical Use
sbb-itb-ed556b0
How the study was designed
Researchers used a prospective cohort design. In plain English, they started with workers who did not have major neck pain at baseline and followed them for 12 months. The goal was simple: find which baseline factors predicted neck disability one year later.
After that, the study tested which of those starting-point factors had the strongest link to disability at 12 months.
Who was included and what was measured at baseline
The cohort focused on full-time workers ages 18–55 in high-risk jobs [1][3]. To be included, participants had to start the study without major neck pain. More specifically, they could not report pain above 30 mm on a 100-mm visual analog scale (VAS) during the three months before enrollment [1][3]. Workers were excluded if they had a history of trauma, spinal surgery, or diagnosed conditions such as fibromyalgia or rheumatoid arthritis.
Baseline data came from questionnaires and physical exams. Trained therapists measured:
- cervical range of motion
- neck flexor endurance
- pressure pain thresholds
Workers also filled out self-administered questionnaires on demographics, pain history, sleep, headaches, perceived muscular tension, and psychological job demands. Researchers recorded workstation ergonomics and neck posture as well [1][3]. All of these baseline measures became candidate predictors in the model.
How long-term neck disability was defined at follow-up
Participants completed monthly self-administered diaries for 12 months. These diaries tracked pain intensity and functional status, which helped separate short-term pain from more persistent work-related disability [1][3].
A worker was counted as having long-term neck disability only if all of the following were present [1]:
- neck pain lasting more than 24 hours
- pain intensity greater than 30 mm on a 100-mm visual analog scale
- no neurologic symptoms
- a Neck Disability Index (NDI) score of at least 5
The NDI is a 10-item questionnaire scored from 0 to 50 that measures functional status [1]. Follow-up was strong: 535 of 559 participants completed the 1-year assessment, for a 96% follow-up rate [1].
Those baseline measures were then tested as candidate predictors of 12-month disability. The next step was to compare which factors carried the most predictive weight.
How the model was built and what predicted disability
Using the baseline measures collected at enrollment, the researchers tested which factors best predicted disability at 12 months. They used penalized logistic regression to build a more stable prediction model and cut down on overfitting. In plain English, that helps keep risk estimates steadier across different high-risk workplaces.
Candidate predictors and final model versions
The candidate predictors covered pain beliefs, work impact, headaches, sleep problems, pain history, functional limits, and mechanical exposure.
From that group, the team built two versions of the model so it could work in both detailed clinical settings and faster workplace screening.
| Model Version | Item Count | Primary Advantage | Practical Use |
|---|---|---|---|
| Full Model | 18 items | Higher precision and broader risk profiling | Detailed clinical assessment and research |
| Simplified Model | 5 items | Easier to use in fast-paced settings | Rapid workplace screening and early triage |
So clinicians can choose the version that fits the moment: a deeper assessment or a quick screen.
The strongest predictors: beliefs, work impact, headaches, and sleep
The strongest predictors were pain beliefs, work interference, headaches, sleep disturbance, and baseline pain intensity. The model also found that neck flexion for most of the workday and whole-body vibration exposure increased risk [4].
How well the model performed
The full 18-item model delivered higher precision for detailed clinical assessment. The 5-item version still kept enough predictive value to support rapid screening in workplace settings [1].
What the findings mean for prevention and clinical care
How workplace teams can use risk estimates earlier
The simplified model makes it easier to spot risk fast. That matters because the best time to step in is often before neck pain starts to derail day-to-day function. A sick-leave period of 4 to 12 weeks is a key window for action. Once time away from work stretches out, the odds of returning to work start to drop [2].
For occupational health teams, that opens the door to earlier screening during routine check-ins, especially when a full assessment isn’t realistic. The study’s simplified 5-item screen can work as a practical first pass. A score of 2 or higher on the 0–4 scale identifies most workers at risk, with 82% sensitivity [1].
In plain terms, this helps teams decide who may need help sooner rather than later. Workers flagged by the screen can be moved up for steps like:
- ergonomic changes
- task rotation
- psychosocial support
That kind of early action can keep a manageable problem from turning into long-term disability. And some fixes are pretty direct. Workers without adjustable seating are more likely to develop neck disability, which makes workstation upgrades one of the clearest employer actions in the study [1].
The same risk signs can also help shape care plans at the clinic level, where treatment can be matched more closely to what each worker is dealing with.
How Portland Chiropractic Group can apply the model in care planning

At Portland Chiropractic Group in Oklahoma City, clinicians can add risk screening to intake visits for workers with neck pain or early warning signs. From there, care can be scaled to fit each worker’s risk profile instead of using the same plan for everyone.
For workers in the high-risk group, early chiropractic assessment can be paired with exercise, education, and work modification. That mix gives care teams a way to address both symptoms and the job factors that may be keeping the problem going.
Predictors at a glance: a reference table
The main predictors and how they may guide care are summarized below.
| Predictor | Category | Intervention It May Guide |
|---|---|---|
| Pain beliefs and muscle tension | Psychosocial | Stress management, micro-breaks, relaxation techniques |
| Work interference and job demands | Work-related | Task rotation, schedule adjustments, functional training |
| Headache frequency | Clinical | Pain management, posture correction, activity pacing |
| Sleep disturbance | Clinical | Sleep hygiene support, workload review |
| Neck flexion posture and whole-body vibration | Biomechanical | Ergonomic workstation assessment, adjustable equipment |
Conclusion: What this study adds for workers, clinicians, and employers
Taken together, these findings show how a risk model can help people act sooner, not later. The model estimates 12-month neck-disability risk by bringing together psychosocial factors, symptoms, and work-exposure factors. In plain English, it gives a more complete picture of who may be headed toward worse neck-related disability over the next year.
One point stands out: risk is shaped by symptoms, sleep, and work impact – not posture alone. That matters. It shifts the focus away from one narrow cause and toward the mix of things that affect how people feel and function day to day. Because of that, the model can help clinicians spot risk earlier, and it can also guide workplace prevention efforts.
For employers, the message is direct: reduce monotony, improve support, and address modifiable work strain early.
FAQs
Who should be screened with this model?
This model is built for workers in high-risk jobs that involve cumulative, repetitive, and sustained physical force.
It helps clinicians and occupational health providers spot the people most likely to develop persistent, moderate-to-severe neck disability over 12 months. The model looks at factors like pain-related beliefs and the ways neck problems spill into daily life, including work, sleep, and headaches.
What does a score of 2 or higher mean?
In this study, the main outcome was an NDI score of 22% or higher at 12 months. The study does not give a separate clinical meaning for a score of 2 on its own.
The NDI is a 10-item questionnaire. Higher percentage scores mean more pain and more trouble with day-to-day function. Put simply, the higher the score, the more neck pain is affecting daily activities and work.
How can this model help prevent long-term neck disability?
This model helps prevent long-term neck disability by spotting high-risk workers early and estimating each person’s risk with more precision.
That gives clinicians and workplace wellness teams a head start. They can plan targeted support sooner, including personalized rehabilitation, ergonomic changes, or psychosocial care. The goal is simple: improve outcomes, help people return to work, and protect long-term function.
Related Blog Posts
- Neck Pain Relief: 5 Professional Treatment Options
- Why are Women More Prone to Wiplash Associated Disorder (WAD) When Compared to Men?
- Effectiveness of Articular and Neural Mobilization for Managing Cervical Radicular Pain: A Systematic Review With Network Meta-Analysis
- Association between cervical MRI findings and patient-reported severity of headache in patients with persistent neck pain: a cross-sectional study

Comments are closed