

If I had to boil this study down to one point, it would be this: for chronic non-specific low back pain, active care usually beats passive care, and the best choice depends on whether I want pain relief now or better function over time.
Here’s the short version:
- Tailored exercise had the strongest result for pain overall, with pain effects as large as SMD -1.61.
- Cognitive Functional Therapy (CFT) stood out for function, with disability effects around SMD -0.89 to -1.00.
- CBT or behavioral support paired with physiotherapy tended to help early, often by the end of treatment or within 2 months.
- Massage and spinal manipulation may help early symptoms, but their effects looked smaller.
- Education alone ranked near the bottom.
- For exercise, programs lasting 16+ weeks and done 6 to 7 times per week ranked highest for pain relief.
- Chronic non-specific low back pain means low back pain lasting 12 weeks or more without a clear specific cause.
So if you’re choosing care, the pattern is pretty simple: use exercise as the base, and if function, fear, or pain behavior are a big part of the problem, add psychological support.
Quick comparison:
| Treatment | Main strength | When it tended to help |
|---|---|---|
| Tailored exercise | Pain relief | More often later |
| CFT | Function and disability | Early to post-treatment |
| CBT + physiotherapy | Pain and function | Early |
| Behavioral therapy + physiotherapy | Pain | Early to mid-term |
| Massage / manipulation | Symptom relief | Early |
| Education alone | Limited effect | Weak overall |
I’d read this study as a timing guide, not just a winner list: some options help first, while others do more after months of steady care.
Nonsurgical Treatment Options for Low Back Pain: What Really Works?
sbb-itb-ed556b0
How the analysis compared conservative treatments
To compare these treatments fairly, the researchers grouped similar therapies and checked results at several follow-up points.
Treatments included in the comparison
The study grouped related conservative treatments so the comparisons would make more sense. Exercise therapy covered core stabilization, resistance training, and motor control exercises. Hands-on treatments included spinal manipulation, dry needling, and massage. Education (Back School) and multidisciplinary biopsychosocial rehabilitation were grouped as education or combined care [3][5]. Multimodal care, which included psychological support plus structured physiotherapy, was looked at as its own category [5].
How outcomes were measured over time
The study tracked two main outcomes: pain intensity and function. Pain intensity was measured with the Visual Analogue Scale (VAS) or Numeric Rating Scale (NRS). Function was measured with tools such as the Roland-Morris Disability Questionnaire (RMDQ) or the Oswestry Disability Index (ODI) [2][5].
Results were recorded across four follow-up windows:
| Follow-up Window | Time Period Post-Treatment |
|---|---|
| Post-intervention | End of treatment to <2 months |
| Short-term | 2 to <6 months |
| Mid-term | 6 to <12 months |
| Long-term | ≥12 months |
These time windows help show when treatment effects showed up, which the next section breaks down by outcome.
What the study found for pain and function
Conservative Treatments for Chronic Low Back Pain: Pain vs. Function vs. Timing
The pattern was pretty clear: active treatments beat passive care or education-only plans. But the size of the effect changed based on the treatment and what researchers were measuring. And timing matters too. Some options help soon after treatment, while others take more time to show their full effect.
Which treatments showed stronger pain reduction
Tailored exercise, including Pilates and McKenzie-based methods, showed the strongest pain relief overall, with a standardized mean difference (SMD) of -1.61 [2]. That was the top result for pain.
Cognitive Functional Therapy (CFT) also performed well. Compared with usual care, it had an SMD of -0.71 [4]. CFT stands out because it works on both movement habits and the psychological side of pain.
Psychological care also helped when it was paired with physical treatment. Behavioral therapy delivered alongside physiotherapy showed a large post-intervention effect on pain, with an SMD of 1.08 [5]. In plain terms, these approaches seem to do more when they sit next to structured exercise, not when they work on their own.
On the other hand, spinal manipulation showed only modest pain relief, with little gain beyond placebo [3][7]. Education alone ranked lowest for pain [4][5].
Which treatments improved function best
Pain and function don’t always move in lockstep. A person may hurt less without moving much better, or move better even if pain still lingers.
That split showed up in the results. CFT, alone or with biofeedback, was one of the strongest options for reducing disability, with an SMD of -0.89 to -1.00 [4]. CBT delivered with physiotherapy also led to a large functional improvement right after treatment, with an SMD of 1.01 [5].
Exercise helped pain more than function. Exercise therapy reduced pain by about 15.2 points on a 0 to 100 scale, but function improved by only about 6.8 points on that same scale [3]. Multidisciplinary care showed a similar pattern: moderate pain relief (SMD -0.55) but only a small gain in function (SMD -0.41) [3].
Comparison table: treatments, outcomes, and timing
The table below lines up the main pain and function results in one place.
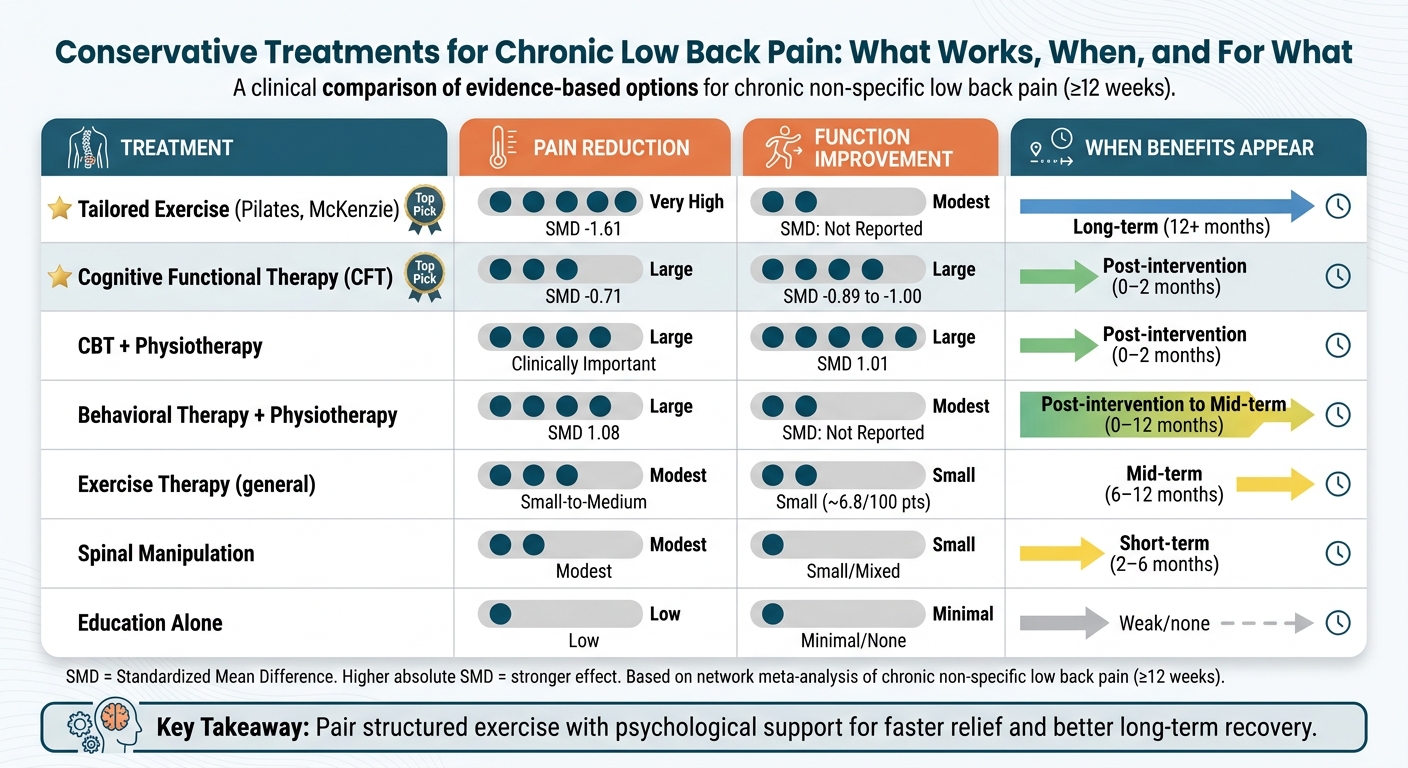
| Treatment | Pain Reduction | Function Improvement | Timing of Benefit |
|---|---|---|---|
| Tailored Exercise (Pilates, McKenzie) | Very high (SMD -1.61) [2] | – | Long-term |
| CFT | Large (SMD -0.71) [4] | Large to very large (SMD -0.89 to -1.00) [4] | Post-intervention |
| CBT + Physiotherapy | Clinically important [5] | Large (SMD 1.01) [5] | Post-intervention |
| Behavioral Therapy + Physiotherapy | Large (SMD 1.08) [5] | – | Post-intervention to mid-term |
| Exercise Therapy | Small to medium [3] | Small [3] | Long-term |
| Spinal Manipulation | Modest [3][7] | Small/mixed [3][6] | Short-term |
| Education Alone | Low [4][5] | – | – |
These differences in timing matter most when the choice comes down to short-term relief versus longer recovery.
When benefits tended to appear
Short-term relief versus longer-term progress
Once you know which treatments did best, the next step is simple: when do they start to help?
The answer depends on the treatment. Some approaches can ease symptoms within a few weeks. Others tend to pay off after months of steady, structured care.
Massage and spinal manipulation were linked with faster symptom relief, which matters early on when pain makes it hard to move [2][6]. CBT plus exercise and pain education plus exercise also improved pain and function within the first two months after treatment [5].
For longer exercise plans, duration and frequency stood out. Exercise programs lasting at least 16 weeks ranked highest for pain relief, and six to seven sessions per week ranked highest among exercise doses [1].
By 6–12 months, behavioral therapy plus physiotherapy continued to reduce pain, while pain education plus physiotherapy led to the strongest lasting gains in function [5].
What this means for choosing a care plan
This timing gap matters most when symptoms are bad enough to limit daily activity.
A good starting point depends on the goal: faster relief or longer-term function. If pain is stopping normal movement, massage, manipulation, or CBT and pain education paired with exercise may ease symptoms soon enough to help someone get moving again.
After that, the evidence points to active, structured exercise as the main long-term plan [2]. Exercise interventions can reduce the three-year recurrence rate of chronic low back pain by about 30% [1]. For people living with lasting disability, Cognitive Functional Therapy, on its own or paired with biofeedback, has shown large drops in disability [4].
The practical point is pretty clear: some treatments help sooner, while others tend to hold up better over time.
Key takeaways for conservative low back pain care
When you put the pain, function, and timing results side by side, a clear pattern shows up: active, combined care beat passive care. But there’s a twist. The top option wasn’t the same for pain and function.
For pain, behavioral therapy plus physiotherapy had the biggest effect right after treatment. For function, Cognitive Functional Therapy and CBT plus physiotherapy led to the biggest gains [4][5].
Timing matters too. Pain education plus physiotherapy held up best for function in the mid-term. And behavioral therapy plus physiotherapy kept meaningful pain relief going through 6 to 12 months [5].
The clearest practical point is simple: pair structured exercise with psychological support when the goal is faster relief and better recovery.
FAQs
How do I choose between pain relief and better function?
Many conservative treatments can improve both pain and function. Adapted physical exercise, multidisciplinary care, and some combined physiotherapy approaches are often among the strongest options for reducing pain and disability.
If pain relief is your main priority, massage and spinal manipulation may help more. But if you want to move better day to day and see longer-lasting gains in function, active approaches like structured exercise and cognitive functional therapy often do more heavy lifting.
What does a time-course network meta-analysis actually show?
A time-course network meta-analysis compares how well different non-surgical treatments work by combining direct and indirect evidence across follow-up periods.
Instead of looking at just one snapshot in time, it shows how pain and function change in the short, medium, and long term. That makes it easier to see which conservative approaches lead to the biggest gains when compared with standard care or other options.
Which conservative treatment is most likely to help first?
For chronic non-specific low back pain, non-drug, non-surgical care should come first. That’s the main starting point.
Research shows that active physiotherapy, especially adapted exercise, is the option most likely to help early. It can reduce pain and improve function, which is often what people care about most day to day.
Multidisciplinary programs and cognitive functional therapy also show strong results. In practice, many people do best with a mix of approaches, such as structured exercise plus pain education.
Related Blog Posts
- Dry cupping therapy combined with conventional therapy does not provide additional benefits over conventional therapy alone in patients with non-specific chronic low back pain: a randomized trial
- Effectiveness of Articular and Neural Mobilization for Managing Cervical Radicular Pain: A Systematic Review With Network Meta-Analysis
- Cost-effectiveness of spinal manipulation, exercise, and self-management for spinal pain
- Recent highlights in low back pain research, Part II: Prevention and management

Comments are closed