

If you have a degenerative meniscus tear, surgery usually does not lead to better 10-year results than exercise-based care.
When I look at the long-term data, the message is plain: pain and function tend to end up about the same with arthroscopic partial meniscectomy (APM) or physical therapy, while surgery may come with a higher chance of joint wear and later knee surgery in some studies.
Here’s the short version:
- Pain and function: At 10 years, APM does not beat structured exercise for most middle-aged and older adults with degenerative tears.
- Sham surgery data: In one 10-year trial, APM showed no meaningful edge over sham surgery for pain or function.
- Arthritis changes: Some studies found more osteoarthritis progression after APM.
- Later surgery risk: In the FIDELITY trial, 12% of the APM group had knee replacement or realignment surgery within 10 years vs. 4% in the sham group.
- Exercise first: A 12-week rehab program is usually the first step.
- When surgery still fits: APM may still have a role if you have a true locked knee or if rehab does not help enough.
If I had to sum up the article in one line, it would be this: for most degenerative meniscal tears, start with rehab, not surgery.
| Topic | What the 10-year evidence shows |
|---|---|
| Pain relief | Similar results with APM and exercise/PT |
| Physical function | Similar long-term function in both groups |
| Osteoarthritis | Surgery does not protect the joint; some data suggest more wear after APM |
| Knee replacement risk | May be higher after APM in some studies |
| Best first treatment | Structured exercise and symptom-guided care |
| Main exception | True mechanical locking |
I’ll keep the rest focused on what these findings mean for your treatment choices, without rehashing every study detail.
Exercise vs Surgery for Degenerative Meniscus Tears
sbb-itb-ed556b0
What 10-Year Studies Show About APM
The big question is simple: if surgeons remove part of the meniscus, does that still help 10 years later?
The long-term data point in the same direction: APM does not show a lasting edge over sham surgery or exercise-based care.
Sham Surgery Trials: No Lasting Advantage for Pain or Function
The FIDELITY trial tested APM against sham surgery. In the sham group, patients went through the same surgical setup, but no meniscal tissue was removed. At the 10-year follow-up, APM showed no clinically important benefit over sham surgery for pain or function [4].
There was another signal worth paying attention to. Later surgery happened more often in the APM group. 12% of patients in the APM group needed knee replacement or realignment surgery within 10 years, compared with 4% in the sham group – roughly three times the rate [4]. Radiographic osteoarthritis progression was also higher after APM: 81% versus 70% in the sham group [4].
"Our findings suggest that this may be an example of what is known as a medical reversal, where broadly used therapy proves ineffective or even harmful." – Teppo LN Järvinen, MD, PhD, University of Helsinki [4]
Exercise-based trials reach much the same place, just by a different route.
Exercise Therapy Trials: Similar 10-Year Results Without Meniscus Removal
The OMEX trial compared APM with a structured exercise therapy program. At 10 years, both groups had improved pain and function, and there was no clinically meaningful difference between them [1].
Exercise therapy led to more strength gains during the first year. But by year 10, that gap had mostly faded. Radiographic osteoarthritis developed in 23% of the APM group and 20% of the exercise group, with no meaningful difference in progression [1].
Bjørnar Berg, PhD, from Oslo University Hospital, put it plainly:
"Exercise therapy should be the preferred treatment over APM for middle-aged individuals with degenerative meniscal tears." [1]
Systematic Reviews and Trials: A Consistent Pattern
The same pattern shows up in bigger reviews. A systematic review of 17 randomized controlled trials involving 2,037 patients found no difference in functional outcomes, pain, or quality of life between APM and physical therapy [5]. The review authors said the gains from APM for degenerative, nonobstructive tears are limited, and that outcomes are similar between surgery and physical therapy [5].
That matters because treatment decisions usually come down to a few practical things: pain, function, arthritis progression, and the odds of needing more surgery later.
Pain, Function, Osteoarthritis, and Knee Replacement Risk at 10 Years
Pain Relief and Function Often Even Out Over Time
When you zoom out to the 10-year mark, the picture stays pretty much the same. Pain and function tend to look similar whether someone had APM or stuck with exercise-based care. Most of the improvement shows up in the first 1 to 2 years, then levels off and stays fairly steady through year 10 [1][3].
That matters because the long-term gap between the two paths is small and not clinically meaningful [1][3]. In plain English: surgery usually doesn’t lead to better day-to-day knee outcomes a decade later. And full symptom relief is uncommon no matter which route a person takes [1].
Osteoarthritis Progression May Be Higher After Meniscus Removal
The structural findings point the same way. When meniscal tissue is removed, cartilage stress can go up, which may speed joint wear [6]. That’s one reason this issue keeps coming up in long-term studies.
By 10 years, X-ray osteoarthritis rates were similar in both groups, so surgery did not show a meaningful structural edge [1]. APM also does not seem to protect the knee joint or slow arthritis when compared with exercise-based care [1][6].
Later Surgery and Knee Replacement Risk
This weak long-term payoff shows up again when you look at later surgery. APM does not seem to reduce the chance of needing more knee surgery down the line, and for some tear types it may be tied to worse long-term results.
For degenerative tears in general, some research suggests the risk of total knee replacement may be up to 5 times higher in patients who undergo APM than in those who follow exercise-based physical therapy [3].
APM vs. Non-Surgical Care: A Practical Comparison
APM Surgery vs. Exercise Therapy: 10-Year Knee Outcomes Compared
Those 10-year findings matter because they change how patients should think about surgery versus rehab. The long-term issue isn’t whether symptoms can get better. It’s which option holds up over time with the fewest downsides.
Structured Exercise and Physiotherapy-Based Rehabilitation
In the trials, rehab usually meant a 12-week progressive program with 2–3 sessions per week [1][7]. These programs focused on strengthening, neuromuscular training, and pacing activity [1][7].
This route usually takes more patience than surgery. Relief tends to come more slowly, and results depend a lot on sticking with the program. Even so, not everyone gets enough relief from exercise alone. About 20% to 32% of patients who start with exercise therapy later choose surgery because symptoms still limit daily life [1][3].
Conservative Care at Portland Chiropractic Group in Oklahoma City

At Portland Chiropractic Group in Oklahoma City, conservative care may include evaluation, manual therapy, supervised exercise, and activity changes based on a patient’s symptoms and goals.
Put simply, the plan should center on three things:
- improving function
- controlling symptoms
- managing long-term knee loading
Comparison Table: APM vs. Non-Surgical Management at Short- and Long-Term Follow-Up
This gap becomes easier to see when both paths are lined up side by side.
| Feature | Arthroscopic Partial Meniscectomy (APM) | Non-Surgical Care (Exercise/PT) |
|---|---|---|
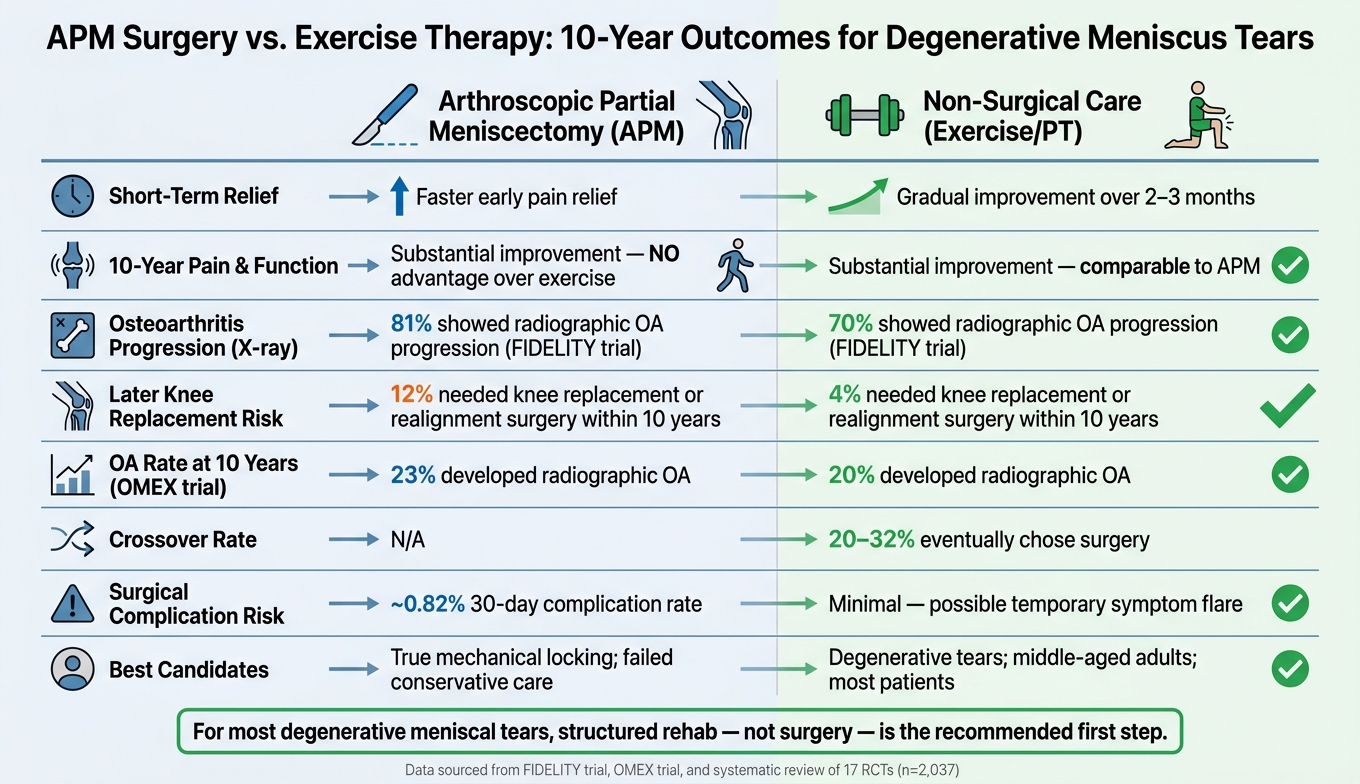
| Short-term relief | Faster early relief [1][3] | Gradual improvement over 2–3 months [7] |
| 10-year pain & function | Substantial improvement; no advantage over exercise [1][7] | Substantial improvement; comparable to APM [1][7] |
| Overall satisfaction | Similar to non-surgical care at long-term follow-up [1][3] | Similar to APM at long-term follow-up [1][3] |
| Surgical risks | Rare complications; about a 0.82% 30-day complication rate [2] | Minimal; possible temporary symptom flare |
| Recovery demand | Outpatient surgery with same-day weight-bearing and home exercises [2] | 12-week supervised program; high adherence required [7] |
| Crossover to surgery | N/A | 20% to 32% eventually choose APM [1][3] |
| Best candidates | True mechanical locking; symptoms that fail to improve with conservative care [2][3] | Degenerative tears; middle-aged adults; minimal baseline OA [1][7] |
"Exercise therapy should be the preferred treatment over APM for middle-aged individuals with degenerative meniscal tears." – Bjørnar Berg, Division of Orthopaedic Surgery, Oslo University Hospital [7]
For most patients, structured rehab is the first step. The tradeoff is pretty plain: surgery may bring faster early relief, while non-surgical care asks for more time and follow-through but leads to similar long-term results. The next issue is figuring out when surgery still makes sense.
What This Means for Treatment Decisions
The 10-year data show no routine edge for APM over structured rehab. So surgery has a much smaller place than many people assume. In plain terms, the main decision is this: Who still needs surgery, and who is better off sticking with conservative care?
When Surgery May Still Be Worth Considering
The clearest reason to get an orthopedic evaluation is true mechanical locking, when the knee cannot fully straighten because tissue is physically blocking it [5]. That’s different from stiffness, soreness, or a knee that feels like it might catch now and then.
It also helps to know that starting with conservative care does not shut the door on surgery later. If you delay APM while you try non-surgical treatment first, that delay does not worsen later surgical outcomes if you decide to move forward [5].
For most other patients, structured rehab should be the default path.
How to Build a Long-Term Conservative Care Plan
A strong long-term plan usually starts with a 12-week supervised exercise program built around progressive neuromuscular work and strength training [7]. That first stretch matters, but it’s only the start. After that, the focus shifts to keeping quadriceps and hamstring strength up over time, since both tend to drop off if you stop working on them [7].
Weight management and activity modification can also lower stress on the degenerative meniscus [5]. That might mean changing how much impact you put through the knee, adjusting workout volume, or dialing back movements that keep flaring symptoms.
Periodic check-ins with a clinician, such as the team at Portland Chiropractic Group in Oklahoma City, can help fine-tune the plan as symptoms and function change over time. That matters because exercise and load management match surgery for 10-year pain and function.
Those are the practical choices that matter at 10 years.
Key Points to Remember
- APM does not improve 10-year pain or function for typical degenerative tears [1].
- Osteoarthritis may progress slightly more after APM [1].
- Surgery still has a narrow role for true locking or failed rehab [5].
FAQs
How do I know if my meniscus tear is degenerative?
Degenerative meniscal tears are common in middle-aged adults. On MRI, they often show up as linear signals that reach one or both surfaces of the meniscus. And symptoms don’t always come from the tear alone. They can also stem from broader changes in the joint.
Clinicians usually make the call using a physical exam and imaging. Common signs include localized joint-line tenderness and an MRI pattern that fits a degenerative tear, often with little joint space narrowing.
What counts as a true locked knee?
A true locked knee happens when part of the meniscus gets physically trapped in the knee joint, which means the leg can’t fully straighten.
That’s a mechanical block, not just stiffness. And it’s more often tied to traumatic tears than degenerative tears.
If I start with physical therapy, can I still have surgery later?
Yes. If physical therapy and other non-surgical care don’t bring enough relief, surgery can still be an option later.
Current recommendations usually suggest trying at least 3 months of conservative care first. Choosing physical therapy at the start does not close the door on surgery later. And over the long run, both approaches have shown similar results for pain and knee function.
Related Blog Posts
- Effectiveness of fascial manipulation® versus eccentric training with static stretching on patellar tendinopathy – A randomized clinical trial
- Lumbar disc herniation: Epidemiology, clinical and radiologic diagnosis WFNS spine committee recommendations
- Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging
- Thigh Muscle Changes in the ACL-Deficient Knee: A 4-Year Longitudinal MRI Study of 1,207 Patients

Comments are closed